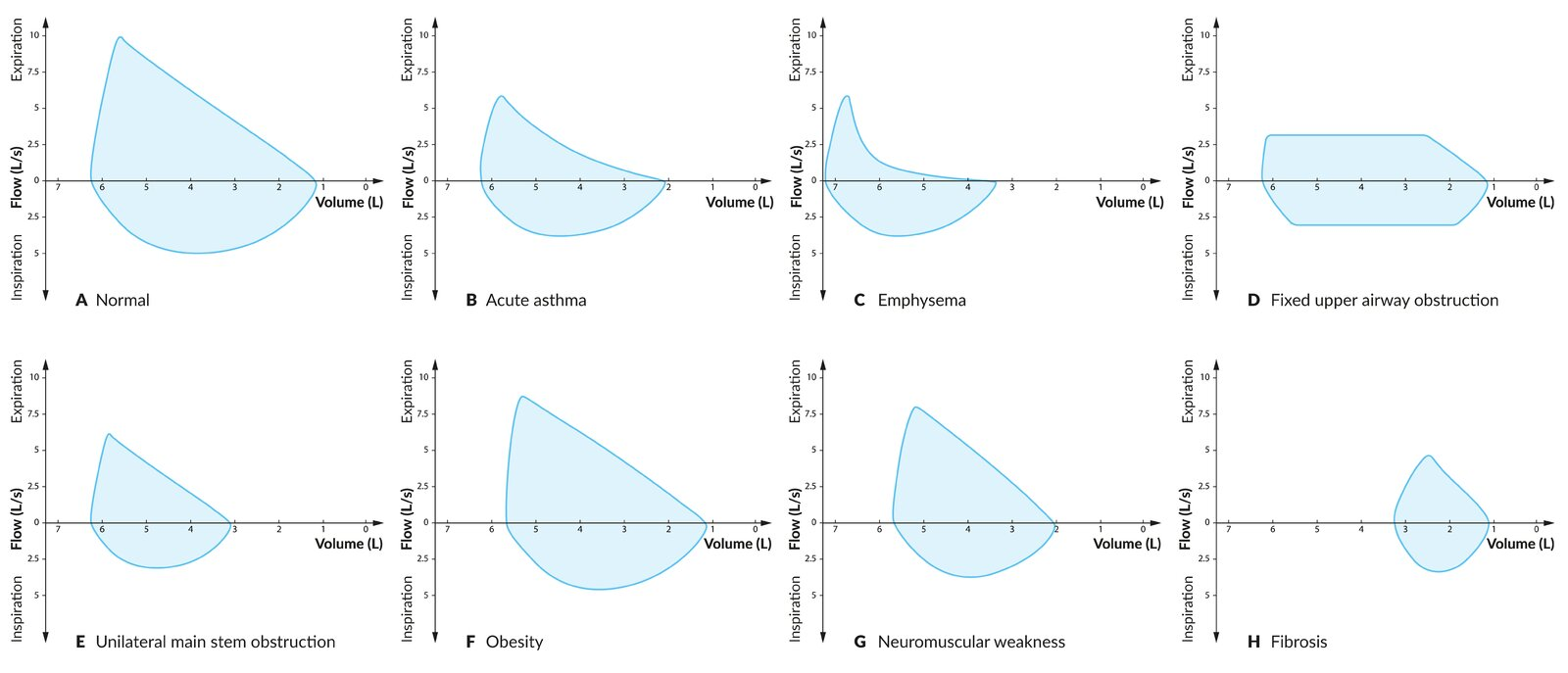
- A flow-volume loop is most commonly used as a graphical representation of spirometry testing. It plots inspiratory and expiratory flow (y-axis) against lung volume (x-axis) during a maximal forced expiration and a maximal inspiration.
- A (normal): At the beginning of the test, the patient has inhaled to total lung capacity of approx. 6.25 L (normal adult range: 6–6.5 L), and there is no flow. As the patient forcefully exhales, the flow quickly reaches a peak at approx. 10 L/s (normal adult range: 6–12.5 L/s) and then declines almost linearly until flow is zero at the residual volume of just over 1 L (normal adult range: 1–1.5 L). The patient then takes a full inspiration to return to total lung capacity.
- B (acute asthma): Expiratory flow is impaired by narrowed airways. Therefore, the peak expiratory flow rate is lower than normal with a slightly concave (scooped) curve toward the residual volume. The residual volume is abnormally elevated, as the narrowed airways have prevented a full expiration.
- C (emphysema): Expiratory flow is obstructed by the collapse of small airways. Therefore, the peak expiratory flow rate is lower than normal with a concave (scooped) curve toward the residual volume. The residual volume and total lung capacity are abnormally elevated due to the lung’s increased compliance, decreased recoil, and air trapping.
- D (fixed upper airway obstruction): Expiratory and inspiratory flows are flattened and reduced, as they are impeded by the fixed obstruction.
- E (unilateral mainstem obstruction): The shape of the loop is normal, but peak expiratory and inspiratory flow rates are reduced, as air can only enter the open portion of the lung. The residual volume is greater than normal because air in the obstructed airway cannot be fully exhaled.
- F (obesity): Expiratory and inspiratory flows and total lung capacity are slightly reduced (compared to diagram A) because of the mechanical limitation of the obese chest wall to expand to full capacity.
- G (neuromuscular weakness): Respiratory muscle weakness results in reduced expiratory and inspiratory flows, reduced total lung capacity, and increased residual volume.
- H (fibrosis): Total lung capacity and peak expiratory and inspiratory flows are substantially decreased due to the lung’s decreased compliance. Note that due to the enhanced elastic recoil of fibrotic lung parenchyma, expiratory flow is not decreased as greatly as lung volume.