A B-cell non-Hodgkin lymphoma (NHL) that typically affects elderly patients in the 7th and 8th decades.
Epidemiology
- Peak incidence: 7th and 8th decades
Etiology
- Gastric MALTomas: multiple studies show an association with H. pylori infection.
- The prevalence of H. pylori infection in low-grade gastric MALTomas is up to 90%.
- Nongastric MALTomas: frequent association with autoimmune conditions
- Salivary gland MALTomas: see Sjogren syndrome
Pathophysiology
The most common trigger for gastric MALT lymphoma is Helicobacter pylori infection, which leads to local recruitment and proliferation of antigen-specific T and B lymphocytes. Over time, chronic immune stimulation results in the emergence of a monoclonal B-cell line that proliferates excessively in the presence of H pylori antigens. This cell line eventually accumulates genetic abnormalities that allow it to proliferate in an antigen-independent fashion, resulting in spread away from the local site of infection.
Clinical features
- Gastric MALTomas
- Present similarly to peptic ulcer disease and gastritis
- Abdominal pain
- Melena, hematemesis, potentially anemia
- Fatigue, weight loss
- Non-gastric MALTomas
- Salivary MALToma: parotid enlargement
Diagnostics
- Histopathology and immunohistochemistry
- Thick infiltrates of small to medium-sized lymphoid cells
- Granulation tissue, ulcerations
- Immunologic phenotyping: markers of B-cell lymphoma (e.g., CD20)
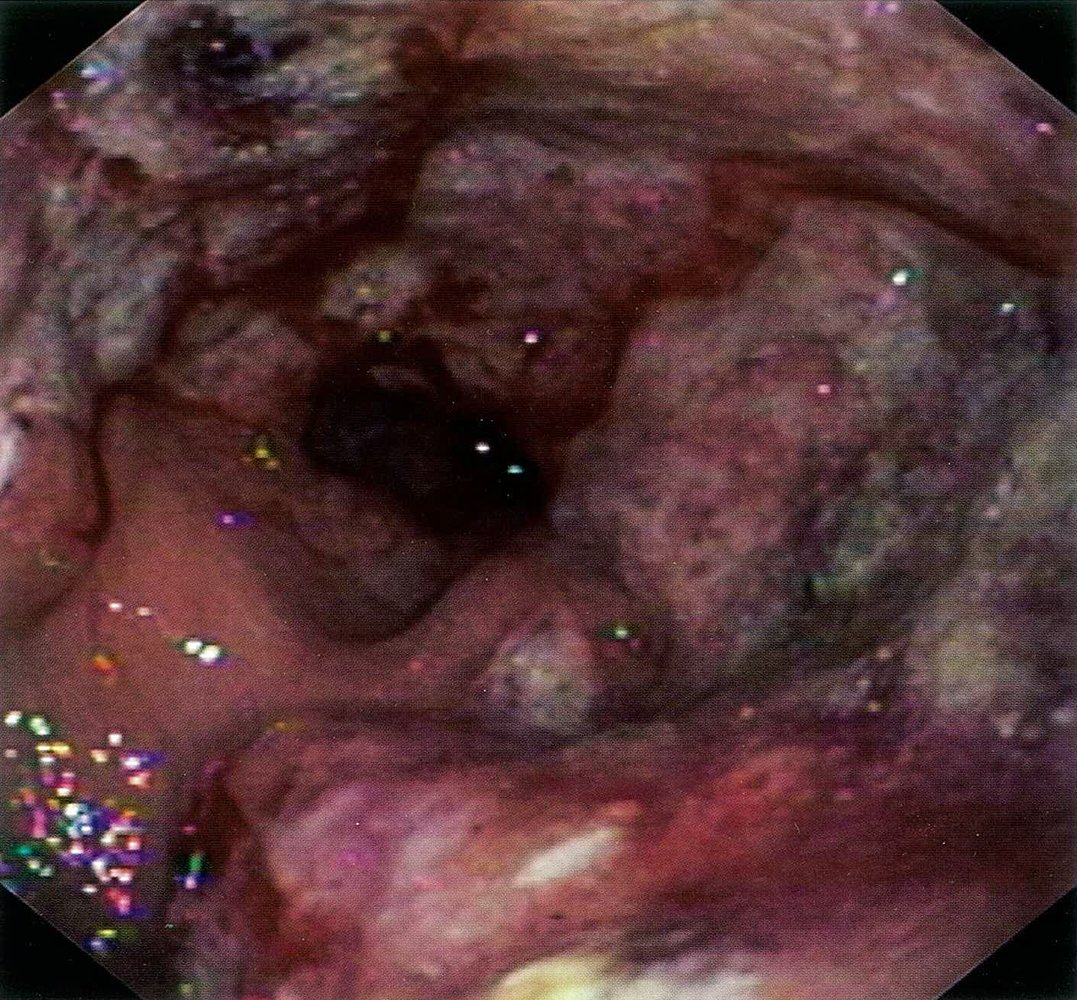
- Endoscopy