Epidemiology
Etiology
Pathophysiology
Clinical features
- BMI: can be normal or slightly elevated
- Central nervous system: Seizures
- As a result of dehydration and electrolyte imbalances (e.g., hyponatremia)
- Cardiovascular symptoms: Cardiac arrhythmias, hypotension
- Mainly caused by potassium deficiency
- As a result of decreased sympathetic nervous system activity
- Gastrointestinal tract
- Esophagitis and/or gastritis
- Esophageal/gastric lacerations (Mallory-Weiss syndrome)
- Bilateral parotid gland swelling (sialadenosis)
- Skin: Calluses on the knuckles (Russell sign)
- Teeth: Caries and perimylolysis due to frequent vomiting
Diagnostics
- ↓ Potassium, ↓ sodium, ↓ chloride, and ↓ calcium
- Metabolic alkalosis
- Possible ↑ serum α-amylase
Differential diagnostics
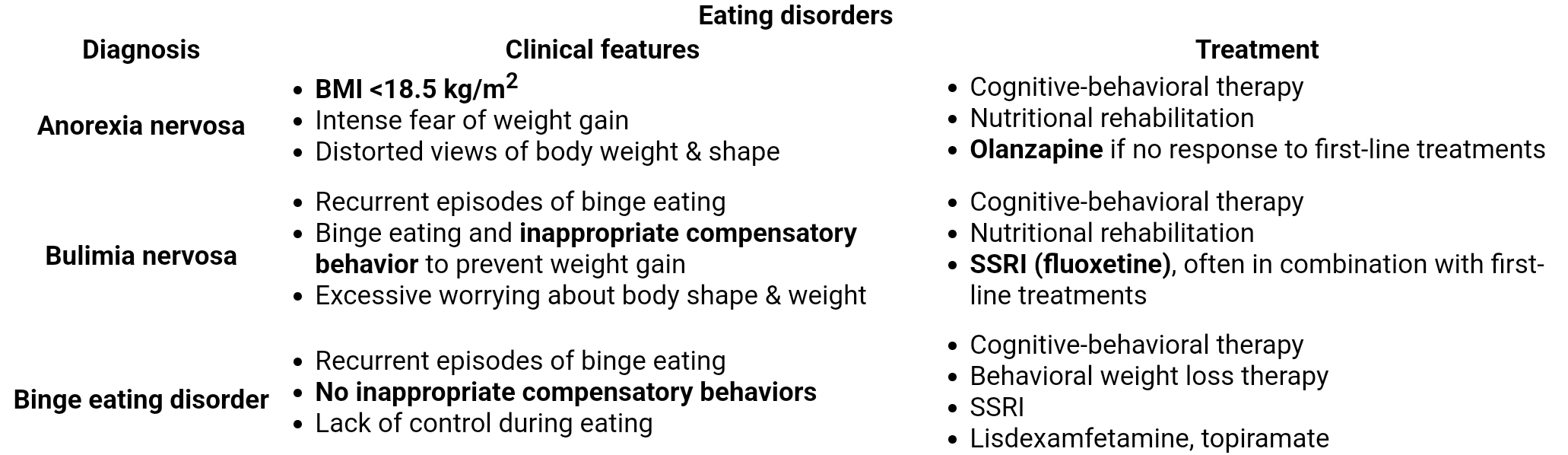
Treatment
- Comanage nutritional management with a dietitian.
- Provide nutritional education.
- Promote healthy eating habits.
- Refer all patients for psychotherapy; consider pharmacotherapy only as adjunctive therapy.
- Preferred initial management in adults: cognitive behavioral therapy with or without an SSRI (fluoxetine)
- Preferred initial management in adolescents and young adults: family-based therapy with an involved caregiver
Pharmacotherapy
- Fluoxetine
- Preferred pharmacotherapy agent for bulimia nervosa
- Can reduce binge eating episodes and purging
Warning
The antidepressant bupropion lowers the seizure threshold and is contraindicated in individuals with a history of anorexia nervosa, bulimia nervosa, or purging behaviors.