Etiology
- Atrial remodeling due to:
- Foci of rapid electrical activity:
- Commonly originate in pulmonary veins
- Alcohol intake & ↑ sympathetic drive may contribute
- Pre-Excited AF: Occurs in pts with Wolff-Parkinson-White (WPW) syndrome (accessory pathway/Bundle of Kent). c
- PE-Induced AFib: The clot blocks the pulmonary artery → acute spike in pulmonary vascular resistance (PVR) → acute Right Ventricle (RV) dilation → acute Right Atrial (RA) stretch. c
Pathophysiology
- The new onset of Afib triggers a vicious circle that can ultimately lead to long-standing Afib with atrial remodeling:
- Afib is triggered by one or both of the following
- Bursts of electrical activity from automatic foci near the pulmonary vein ostia (left atrium) or in diseased, fibrotic atrial tissue
- Pre-excitation of the atria as a result of aberrant pathways (e.g., WPW syndrome)
- Afib is sustained by re-entry rhythms and/or rapid focal ectopic firing
- Re-entry rhythms are more likely to occur with enlarged atria, diseased heart tissue, and/or aberrant pathways (e.g., WPW syndrome).
- Atrial remodeling
- Electrophysiological changes in the atria occur within a few hours of Afib onset (electrical modeling).
- If Afib persists, atrial fibrosis and dilatation (structural remodeling) occur within a few months.
- Electrical and structural remodeling increase susceptibility to Afib, resulting in a vicious circle.
- Afib is triggered by one or both of the following
- Effects of Afib
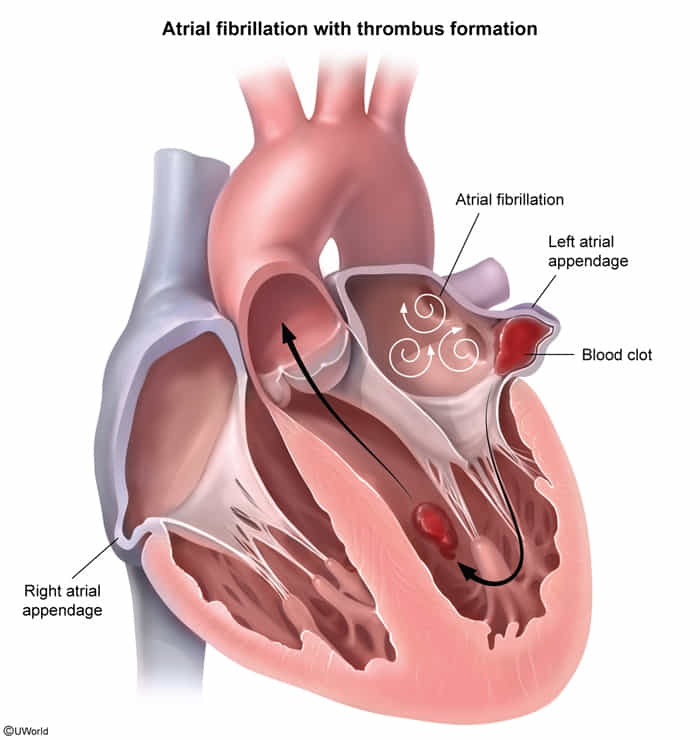
- The atria contract rapidly but ineffectively and in an uncoordinated fashion → stasis of blood within the atria, especially in atrial appendage → risk of thromboembolism and stroke
- Irregular activation of the ventricles by conduction through the AV node → tachycardia
- The atria contract rapidly but ineffectively and in an uncoordinated fashion → stasis of blood within the atria, especially in atrial appendage → risk of thromboembolism and stroke
Clinical features
- Often asymptomatic (incidental finding).
- Sx: Palpitations, fatigue, dyspnea, lightheadedness.
Diagnostics
Atrial flutter vs atrial fibrillation
Link to original
Feature Atrial Flutter Atrial Fibrillation Site of Origin Right Atrium (re-entrant circuit involving the cavotricuspid isthmus). Left Atrium (ectopic foci, most commonly near the pulmonary vein ostia). Pathophysiology Organized macro-reentrant circuit. Chaotic multiple atrial foci. ECG Rhythm Regular or regularly irregular. Irregularly irregular. Atrial Waves (ECG) “Sawtooth” flutter waves (~300 bpm). Fibrillatory waves (no P waves). Management Pearl Catheter ablation is highly curative. Lifelong anticoagulation (CHA₂DS₂-VASc score) is key to prevent stroke.
ECG
Tip
Key: A narrow-complex, irregularly irregular rhythm with no distinct P waves is AFib, regardless of whether classic f-waves are visible on the baseline.
- Coarse AFib: Shows visible, chaotic baseline undulations, typically best seen in leads V1 or II.
- Fine AFib: The baseline appears nearly flat (as seen in this Lead V5 strip). This happens when the chaotic atrial electrical activity is too low-amplitude to register clearly. It is extremely common, especially in leads farther from the atria or in patients with long-standing AFib and atrial scarring.

QRS complex
- Typically narrow QRS complex (< 0.12 seconds)
- Wide QRS complex may be seen in some situations:
- Aberrant conduction, e.g., bundle branch block or preexcitation (as seen in Afib with WPW)
- Complete AV block with a ventricular escape rhythm
- Ashman phenomenon: intermittent aberrant ventricular conduction results in isolated or short runs of wide QRS complexes

Warning
Wide QRS complex may indicate preexcited Afib or aberrant conduction.
Workup
- Transthoracic Echocardiogram (TTE): Assess LA size, LV function, valvular dz, intracardiac thrombus.
- Expected: LA enlargement (remodeling) c , Mitral Stenosis or Mechanical Valve, HFrEF (EF < 40%),
- Labs: TSH (r/o hyperthyroidism), CMP (K+, Mg2+, renal function), CBC.
- Troponins: Only if ACS suspected (ischemia can be cause or result).
CHA2DS2-VASc score
- Purpose: Estimates thromboembolic (stroke) risk in patients with non-valvular Atrial Fibrillation (AFib) to guide the initiation of systemic anticoagulation.
Scoring system
- C - CHF or LVEF 40% (+1)
- H - Hypertension (+1)
- A - Age 75 years (+2)
- D - Diabetes Mellitus (+1)
- S - Stroke, TIA, or prior thromboembolism (+2)
- V - Vascular disease (prior MI, PAD, or aortic plaque) (+1)
- A - Age 65–74 years (+1)
- Sc - Sex category (Female) (+1)
Treatment Thresholds
- 0 (M) or 1 (F): No therapy.
- 1 (M) or 2 (F): Consider oral anticoagulation based on shared decision-making (consider patient preference, bleeding risk).
- 2 (M) or 3 (F): Oral anticoagulation is recommended.
Treatment
- Hemodynamically Unstable (Hypotension, AMS, pulmonary edema, active ischemia):
- Immediate Synchronized Cardioversion. c
- Hemodynamically Stable:
- Rate Control (Preferred initial strategy for most): Target HR < 110 bpm.
- Beta-blockers (e.g., Metoprolol).
- Non-dihydropyridine CCBs (Diltiazem, Verapamil) - Avoid in HFrEF. c
- Digoxin (used if pt has borderline BP or concurrent HFrEF).
- Rhythm Control (Indicated if symptomatic despite rate control, younger pts, or HF exacerbated by AFib):
- Antiarrhythmics (Amiodarone, Flecainide, Sotalol).
- Elective synchronized cardioversion (Must r/o LA thrombus via TEE or ensure 3 weeks of therapeutic anticoagulation prior).
- Catheter ablation (if refractory).
- Rate Control (Preferred initial strategy for most): Target HR < 110 bpm.
Pre-Excited AF
- Tx of Choice: Procainamide or Ibutilide (Chemical cardioversion). c
- CONTRAINDICATED (“ABCD”): Adenosine, Beta-blockers, Calcium channel blockers, Digoxin.
- Why? Blocking the AV node removes the refractory “braking” mechanism, forcing all 300+ atrial impulses down the accessory pathway, rapidly degenerating into Ventricular Fibrillation (VF).
- Anticoagulation (Stroke Prevention):
- Assess stroke risk using CHA2DS2-VASc score (CHF, HTN, Age 75 [2 pts], DM, Stroke/TIA/TE [2 pts], Vascular dz, Age 65-74, Sex category [Female]).
- Score 2 (Men) or 3 (Women): Oral anticoagulation indicated.
- DOACs (Apixaban, Rivaroxaban, Dabigatran): First-line for non-valvular AFib. c
- Warfarin: ONLY indicated for “Valvular AFib” (moderate-to-severe mitral stenosis or mechanical heart valve).