Epidemiology
Etiology
- Cumulative UV exposure (from the sun or from tanning beds) is the most significant risk factor
Pathophysiology
Clinical features
- Precursor and early lesions
- Precursor lesions (actinic keratosis) and in situ lesions (Bowen disease) typically manifest as a enlarging, rounded nodule with rough (keratinized) surface ± ulceration, crusting and bleeding
- Commonly on sun-exposed skin

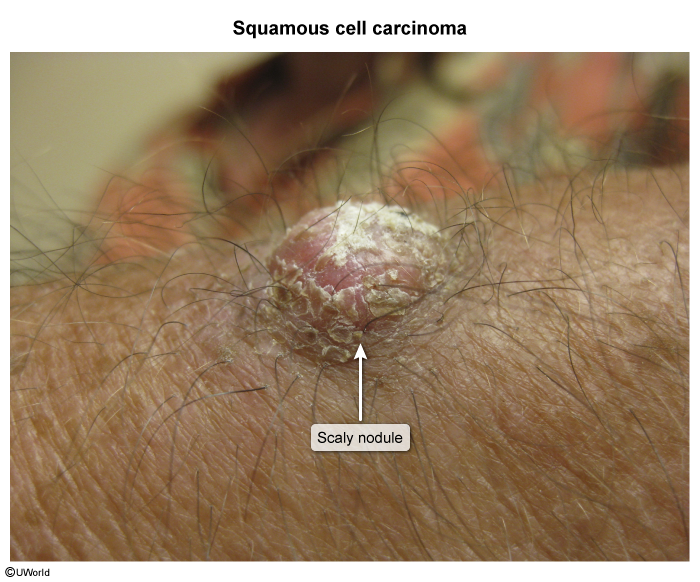
- Invasive cSCC
- Easy friability (i.e., bleeds easily after minor trauma)
- Central ulceration
- Typically occurs on sun-exposed areas
- Metastatic cSCC
- Most common sites for metastasis include lymph nodes (80%)
Diagnostics
Pathology
cSCC occurs as a result of malignant transformation of keratinocytes in the stratum spinosum (prickle cell layer) of the epidermis. These atypical keratinocytes appear as enlarged, polygonal cells with nuclear pleomorphism and atypical mitoses.
- Sheets or nests of malignant keratinocytes
- Keratinization (eg, keratin pearls) & intercellular bridges
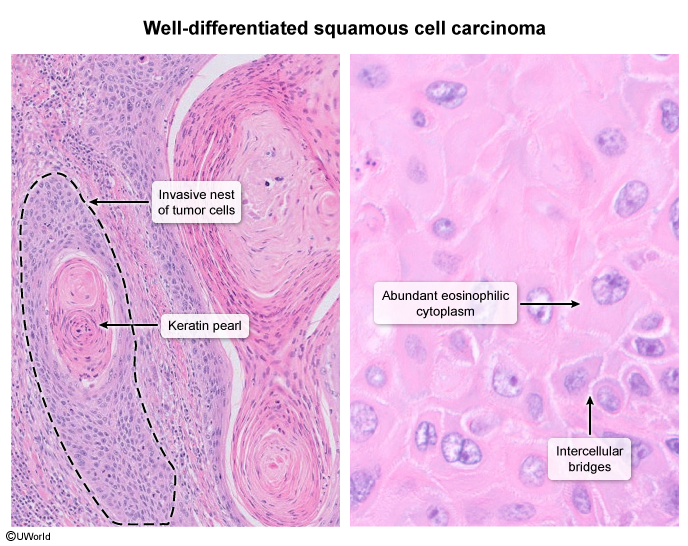
- Keratin pearls: An abnormal structure formed by concentric layers of epithelial cells surrounding a keratin matrix secreted by the cells. Associated with well-differentiated squamous cell carcinoma.
Differential diagnostics
| Feature | Basal Cell Carcinoma (BCC) | Cutaneous Squamous Cell Carcinoma (cSCC) |
|---|---|---|
| Origin | Basal cells in the epidermis | Squamous cells in the epidermis |
| Common Locations | Sun-exposed areas: face, neck | Sun-exposed areas: face, ears, neck, lips, back of the hands |
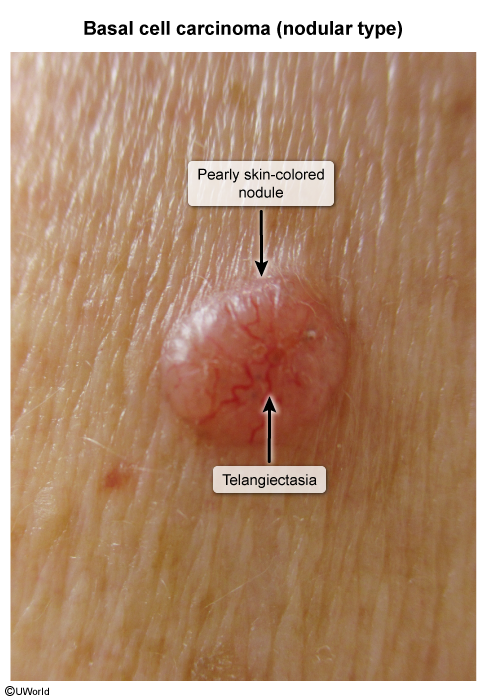
| Appearance | Pearly or waxy bump, flat flesh-colored or brown scar-like lesion | Firm, red nodule, flat lesion with a scaly, crusted surface |
| Growth Rate | Slow-growing | Can be faster-growing than BCC |
| Risk of Metastasis | Rare, low risk | Higher risk compared to BCC |
| Common Causes | Chronic sun exposure, fair skin | Chronic sun exposure, fair skin, history of burns or radiation exposure |
| Typical Age Group | Older adults | Older adults |
| Prevalence | Most common type of skin cancer | Second most common type of skin cancer |
| Treatment Options | Surgical removal, topical medications, radiation therapy | Surgical removal, topical medications, radiation therapy, chemotherapy for advanced cases |
| Prognosis | Generally good if detected early | Good if detected early; can be aggressive if untreated |
- Nodular BCC classically has a translucent or pearly appearance, often with central telangiectasias.
- Cutaneous SCC classically has a rough or scaly (keratinized) surface