Pathophysiology
Colorectal carcinogenesis pathways (molecular pathology)
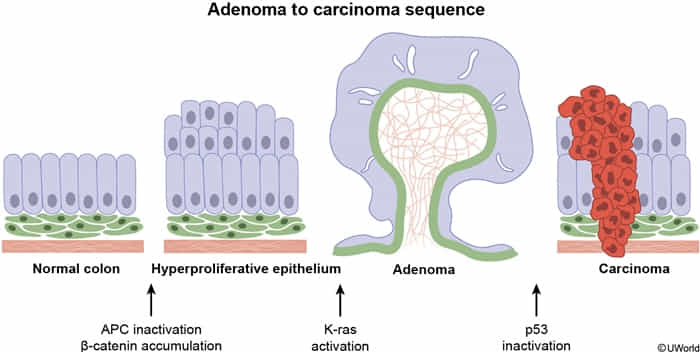
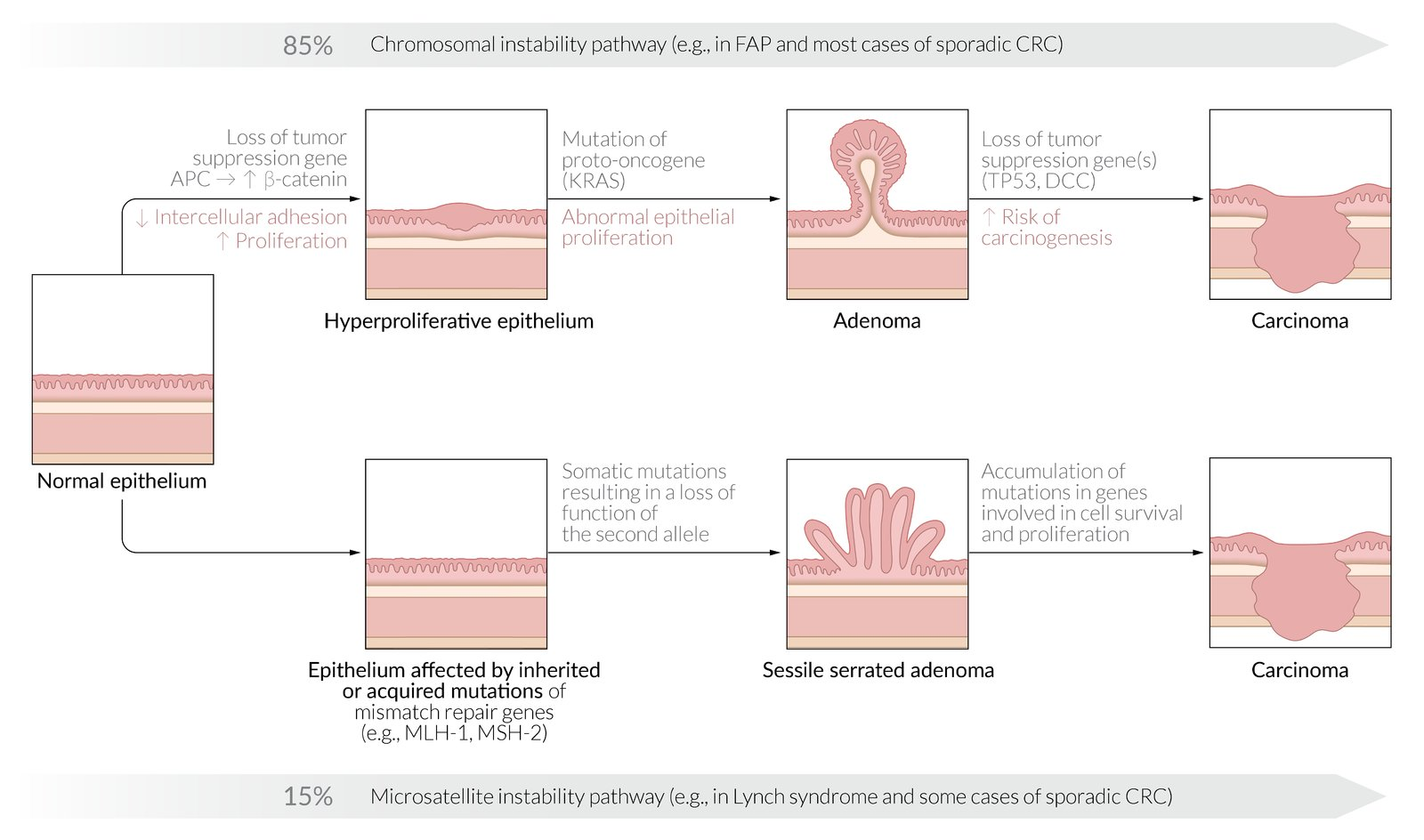
- 1. Chromosomal Instability (CIN) Pathway (~80%)
- The classic Adenoma-to-Carcinoma Sequence.
- Stepwise accumulation of key mutations:
- APC loss (initiation, ↑β-catenin)
- KRAS mutation (unregulated growth)
- p53 loss (malignancy)
- Clinical Association:
- Sporadic CRC (most common).
- Familial Adenomatous Polyposis (FAP): Germline mutation in APC.
Mnemonic
This follows the alphabet: APC → KRAS → P53
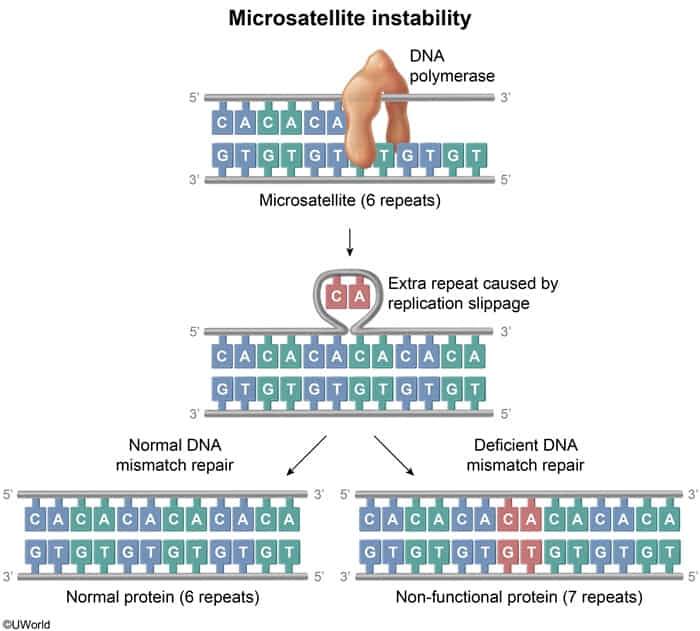
- 2. Microsatellite Instability (MSI) Pathway (~15%)
- Caused by defective DNA Mismatch Repair (MMR).
- Microsatellites are short, repetitive DNA sequences (e.g., CACACA…). During DNA replication, these regions are prone to errors (insertions/deletions).
- Due to mutations in MLH1, MSH2, MSH6, PMS2.
- Leads to errors in repetitive DNA sequences (microsatellites).
- Associated with Lynch Syndrome (HNPCC) and right-sided tumors.
- 3. Serrated Pathway (~5%)
- Arises from serrated polyps.
- Driven by BRAF mutation followed by CIMP (CpG Island Methylator Phenotype).
- CIMP hypermethylates and silences genes, often including the MLH1 mismatch repair gene, which can lead to MSI.
- COX-2 overexpression
- Associated with colorectal cancer
- Possible protective effect of long-term use of aspirin and other NSAIDs
Etiology
Risk factors for colorectal cancer
- Hereditary syndromes
| Syndrome | Gene Mutation | Colon Cancer Risk | Other Associated Neoplasms |
|---|---|---|---|
| Familial adenomatous polyposis | APC | 100% | Upper gastrointestinal, Thyroid, Desmoids/osteomas |
| Lynch syndrome | MSH2/6, MLH1 | 50%-80% | Endometrial, Ovarian |
| Peutz-Jeghers syndrome | STK11 | 39% | Upper gastrointestinal, Pancreatic, Breast |
- Associated conditions
- Inflammatory bowel disease: chronic inflammation → hyperplasia → non-polypoid dysplasia → neoplasia
| Characteristics | Colitis-associated | Sporadic |
|---|---|---|
| Age | Younger (age 40-55) | Older (age >60) |
| Origin of dysplasia | Flat (nonpolypoid) lesions | Polypoid lesions |
| Location | Proximal > distal (particularly with CD) | Distal > proximal |
| Tumors | Multifocal | Singular |
| Histology | Mucinous and/or signet ring cells, Poorly differentiated | Rarely mucinous, Well differentiated |
| Mutations | Early p53 mutation, Late APC gene mutation | Early APC gene mutation, Late p53 mutation |
Pathophysiology
Clinical features
Right-sided colon carcinomas
- Large, bulky masses that protrude into the colonic lumen due to the relatively large caliber of the ascending colon
- Occult bleeding or melena
- Manifestations of iron deficiency anemia (due to chronic bleeding)
Left-sided colon carcinomas
- Often infiltrate the wall of the colon, encircling it and narrowing the lumen
- More likely to cause obstruction
- Changes in bowel habits (size, consistency, frequency)
- Blood-streaked stools
- Colicky abdominal pain (due to obstruction)
- Bowel obstruction occurs earlier in left-sided colon carcinomas because the distal colon has a smaller lumen than the proximal colon and contains solid fecal matter.