Epidemiology
Age: children < 2 years
Etiology
Primary VUR (most common type)
Short intramural ureter → vesicoureteric junction (VUJ) fails to close completely during bladder contraction → VUR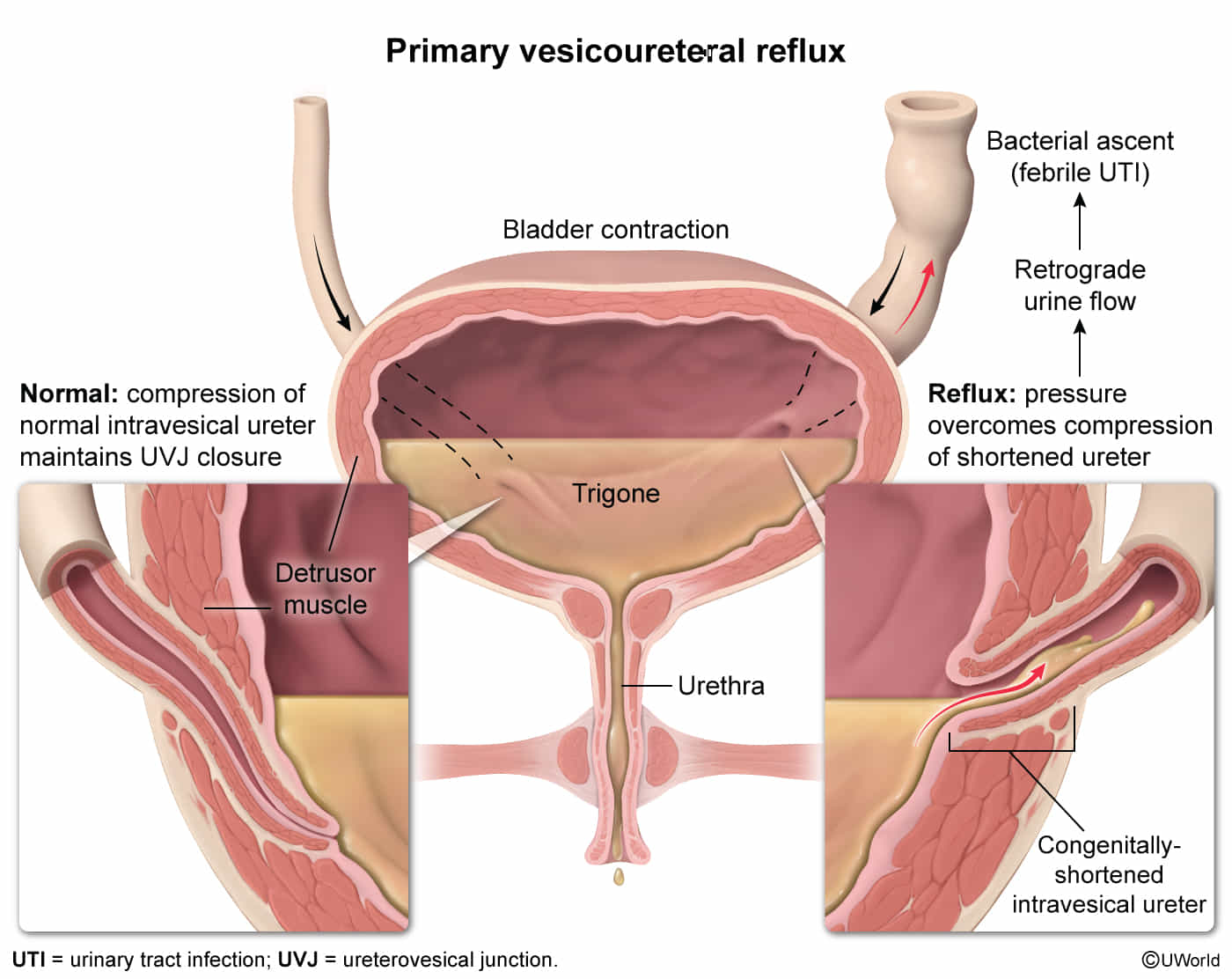
Secondary VUR
- Bladder outlet obstruction (anatomic/functional): high pressure within the bladder → reflux of urine through the VUJ
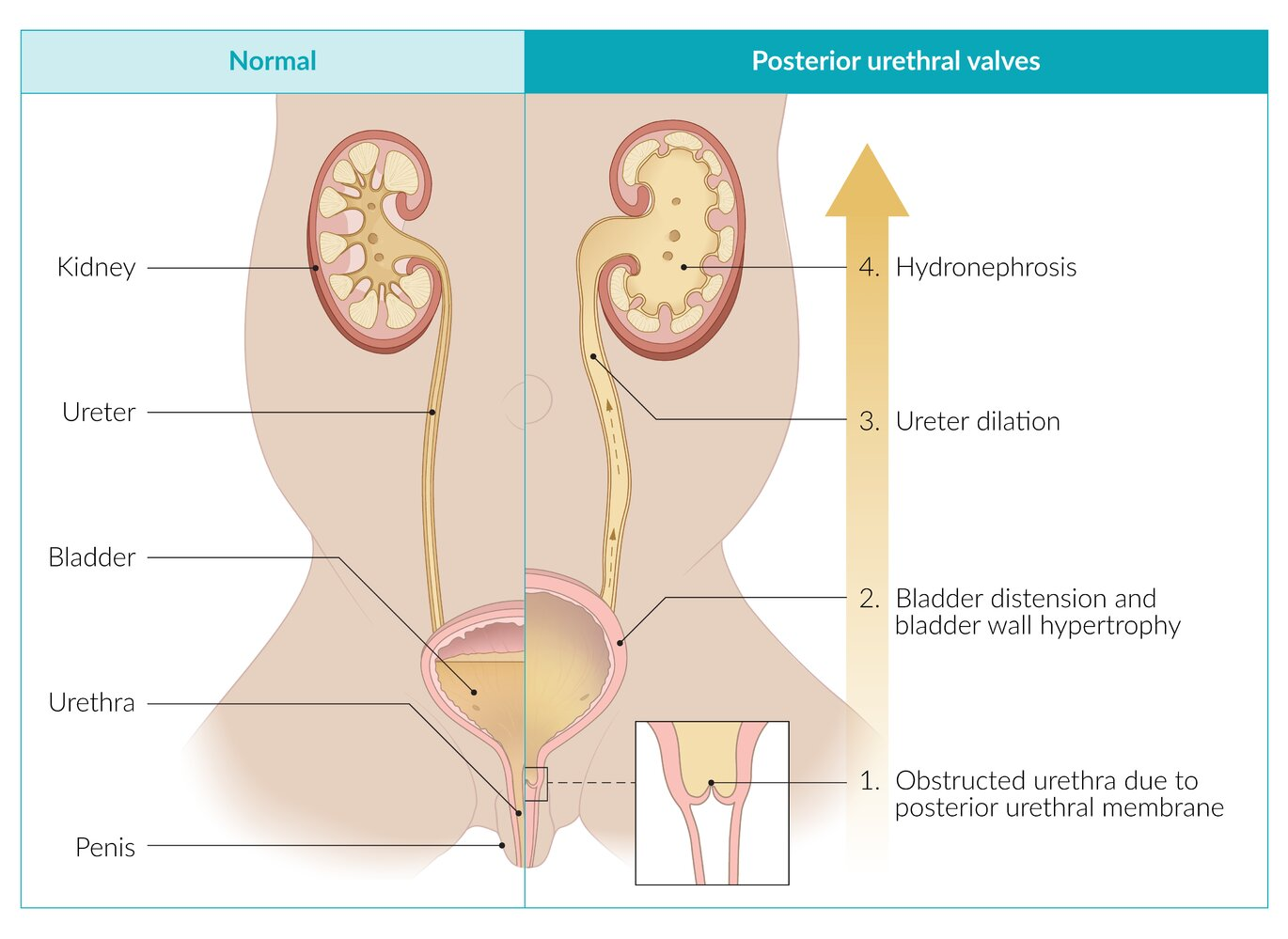
- Anatomic: posterior urethral valves ; urethral meatal stenosis
Pathophysiology
Clinical features
- Suspected in the prenatal period when hydronephrosis is detected on routine antenatal ultrasound
- Postnatal presentation
- Recurrent febrile urinary tract infections
- Neonates: irritability, fever, and listlessness
- Older children: urinary urgency, frequency, incontinence, and dysuria associated with fever
- Reflux nephropathy : renovascular hypertension, kidney failure, uremia
- Recurrent febrile urinary tract infections
- Primary VUR: often spontaneous resolution
- Mechanism: As child grows, intravesical ureter lengthens → creates longer submucosal tunnel → improved valve function → competent VUJ
Tip
VUR is generally asymptomatic until it causes a urinary tract infection.
Diagnostics
Treatment
Spontaneous resolution occurs in most patients with mild VUR, because the intravesical ureter length increases with patient growth.