90% of affected individuals are postmenopausal women.
More common in patients with preexisting mental illness
Etiology
Pathophysiology
Emotional/physical stress → activation of the sympathetic nervous system → massive catecholamine discharge → cardiotoxicity, multivessel spasms, and dysfunction → myocardial stunning
A state of abnormal regional LV wall motion that persists for hours to weeks following transient ischemia
Clinical features
Patients typically have chest pain that can mimic a myocardial infarction and may also have symptoms of heart failure (eg, dyspnea, lower extremity swelling).
ECG often shows evidence of ischemia (eg, ST elevation, T-wave inversion) in the anterior precordial leads; however, coronary angiography typically reveals an absence of obstructive coronary artery disease.
The condition usually resolves within several weeks with supportive treatment only.
Diagnostics
Echocardiography (TTE)
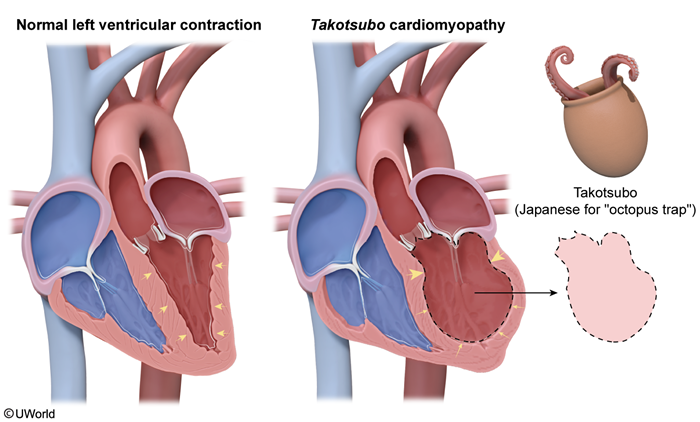
Global LV dyskinesis involving the apex (most common)
Regional wall motion abnormalities
Apical left ventricular ballooning (not always present)