Epidemiology
Etiology
Mechanism
- Normal bone develops a fracture as a result of bone remodeling due to repetitive microtrauma.
Risk factors
- Participation in repetitive high-intensity physical activity: often seen in athletes and military recruits, and children and adolescents participating in year-round sports
- Improper technique during physical activity
- Ill-fitting footwear
- Poor nutrition and/or low calorie intake (e.g., in anorexia nervosa)
- Low bone mineral density (e.g., from bisphosphonate use)
- Calcium and/or vitamin D deficiency
- Female sex
Tip
The female athlete triad syndrome is associated with an increased risk of stress fractures.
Pathophysiology
Clinical features
- Lower extremities (most common): tibia, tarsal navicular, metatarsals (march fracture), femur, fibula, pelvis
- Pain that worsens with activity and resolves with rest
- Focal bone tenderness, erythema, and/or soft tissue swelling
Diagnostics
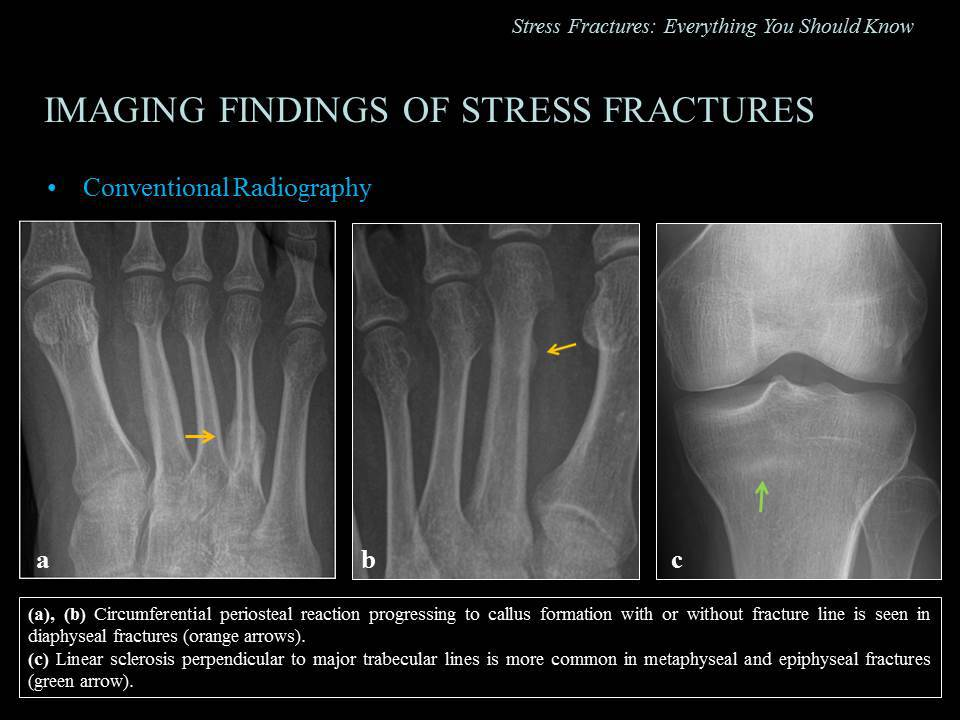
- X-ray: recommended initial imaging study
- Radiographic features of stress fractures include:
- Fracture line: line of faint lucency
- Indirect features: periosteal thickening, increased cortical density, formation of a callus, endosteal thickening and/or sclerosis
- Often normal in the first 2–3 weeks of disease onset
- Radiographic features of stress fractures include:
Treatment
<% tp.file.cursor() %>