Epidemiology
- Most commonly affects individuals from the Mediterranean region to eastern Asia, with the highest prevalence observed in Turkey and Japan
Etiology
- Possible autoimmune and infectious triggers (e.g., precipitating HSV or parvovirus infection)
- Strong HLA-B51 association
Pathophysiology
- Autoimmune systemic vasculitis that can involve arteries and veins of all sizes
- Characterized by the deposition of immune complexes, proliferation of CD4+ T cells, and increased cytokines
Clinical features
- Recurrent painful oral aphthous ulcers (95–100%)
- Typically the initial presenting symptom
- Usually last about 1–4 weeks
- Recurrent genital ulcerations (60–90%)
- Ocular disease (50–80%)
- Uveitis (iridocyclitis, chorioretinitis), keratitis, and/or retinal vasculitis
- Skin lesions (35–85%)
- Erythema nodosum
- Positive pathergy skin test: the appearance of an erythematous papule or pustule 48 hours after a 5 mm skin prick with a 20-gauge needle (usually on the forearm)
- The main reason is subcutaneous vasculitis and high sensitivity reaction of the skin.
- Arthritis (30–70%)
Mnemonic
PATHERGY: Positive pathergy test, Aphthous oral ulcers, Thrombosis (arterial and venous), Hemoptysis (pulmonary artery aneurysm), Eye lesions (uveitis, retinal vasculitis), Recurrent Genital ulcers, Young at presentation (3rd decade)
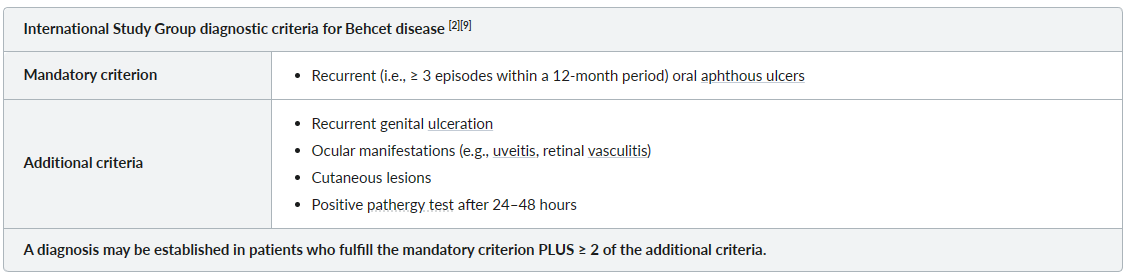
Diagnostics