Epidemiology
- Age of onset: 60–80 years
Etiology
Exogenous risk factors
- Smoking (strongest risk factor)
- Considered to be one of the leading causes of pancreatic cancer and associated with an up to 6-fold increase in the risk of developing malignancy.
- Chronic pancreatitis (especially when present for more than 20 years)
- High alcohol consumption
- Type 2 diabetes mellitus
Endogenous risk factors
- Age > 50 years
- Inherited genetic syndromes (10% of pancreatic cancers)
- Familial atypical multiple mole melanoma (FAMMM) syndrome
- Hereditary breast and ovarian cancer syndrome (BRCA1 and BRCA2 mutations)
- HNPCC
- Von-Hippel-Lindau syndrome
- Neurofibromatosis type 1
- Multiple endocrine neoplasia type 1
- Familial pancreatic carcinoma
Clinical features
In most cases, there are no early symptoms suggestive of pancreatic cancer.
Gastrointestinal symptoms
- Belt-shaped epigastric pain which may radiate to the back
- Nausea
- Malabsorption, diarrhea (possibly steatorrhea secondary to exocrine pancreatic insufficiency)
- Jaundice caused by obstruction of extrahepatic bile ducts (especially in tumors of the pancreatic head)
- Courvoisier sign: enlarged, nontender gallbladder and painless jaundice
- Pale stools, dark urine, and pruritus
Hypercoagulability
- Trousseau syndrome: superficial thrombophlebitis (in 10% of cases)
- Recurring thrombophlebitis in changing locations (migratory)
- Red, tender extremities
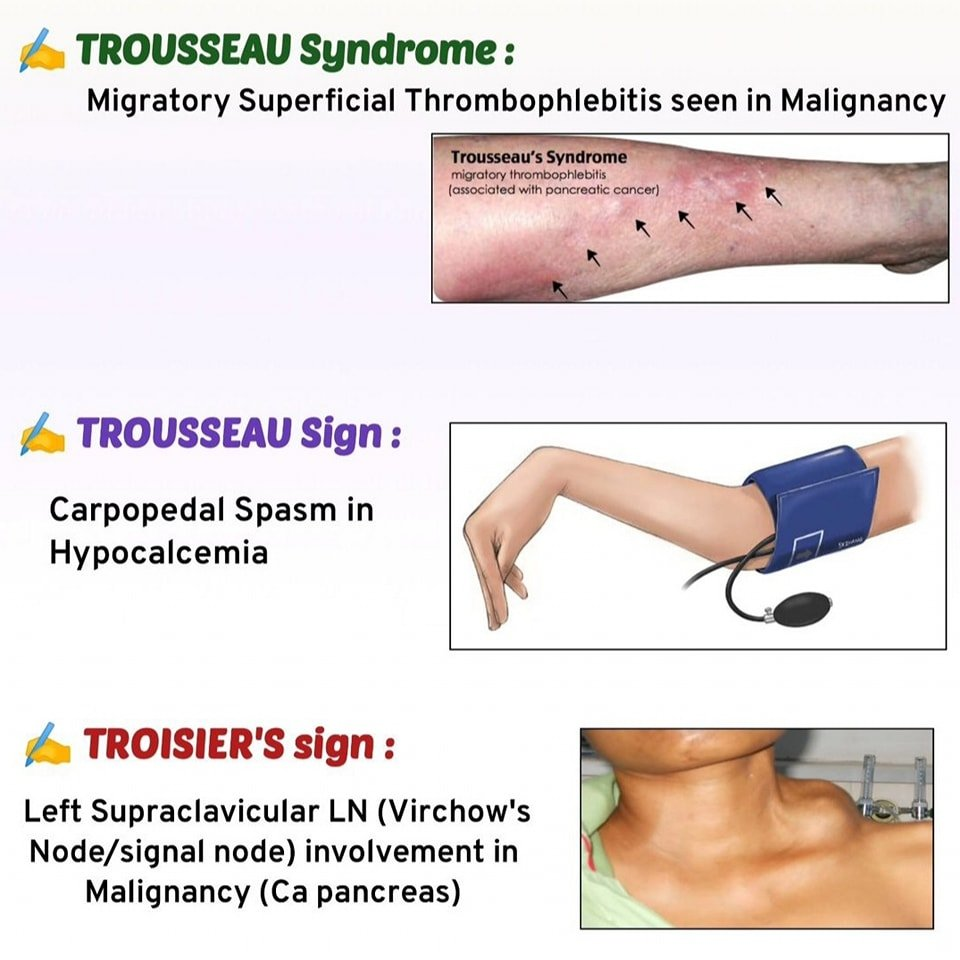
- Classically associated with pancreatic cancer
- The mucin compounds produced by adenocarcinomas have been found to interact with the selectin family of adhesion molecules, leading to thrombocyte activation and aggregation
Tip
A thrombosis of unknown origin may be caused by an undiagnosed malignancy (especially pancreatic cancer, but also pulmonary, and prostatic carcinoma, the “3P’s”).
Warning
In the majority of instances, pancreatic cancer is diagnosed in symptomatic patients once it has already spread regionally or distally and is no longer resectable.
Pathology
Location
- Pancreatic head: 65% of cases
- Pancreatic body and tail: 15% of cases
- Diffuse: 20% of cases
Cell origin
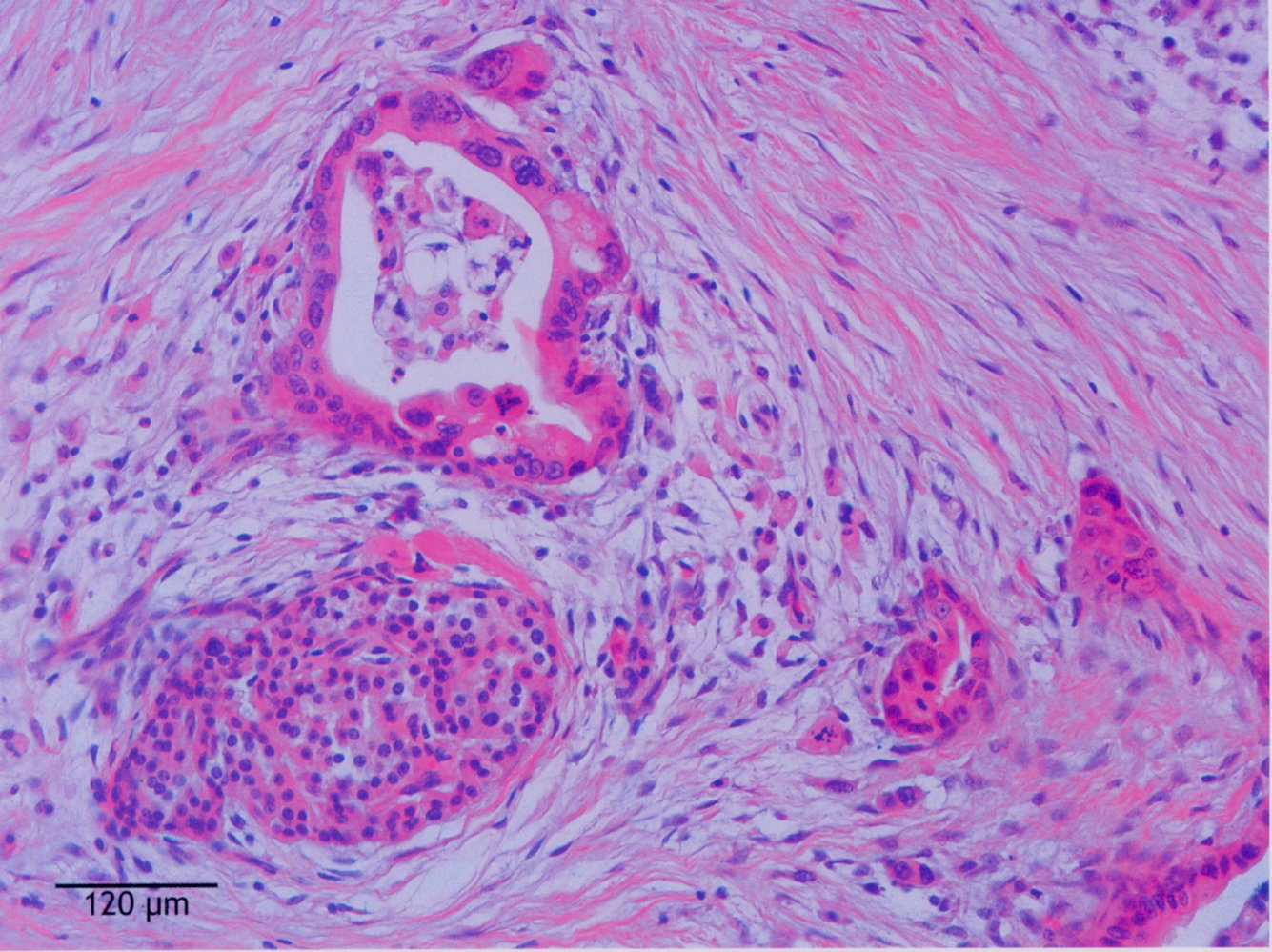
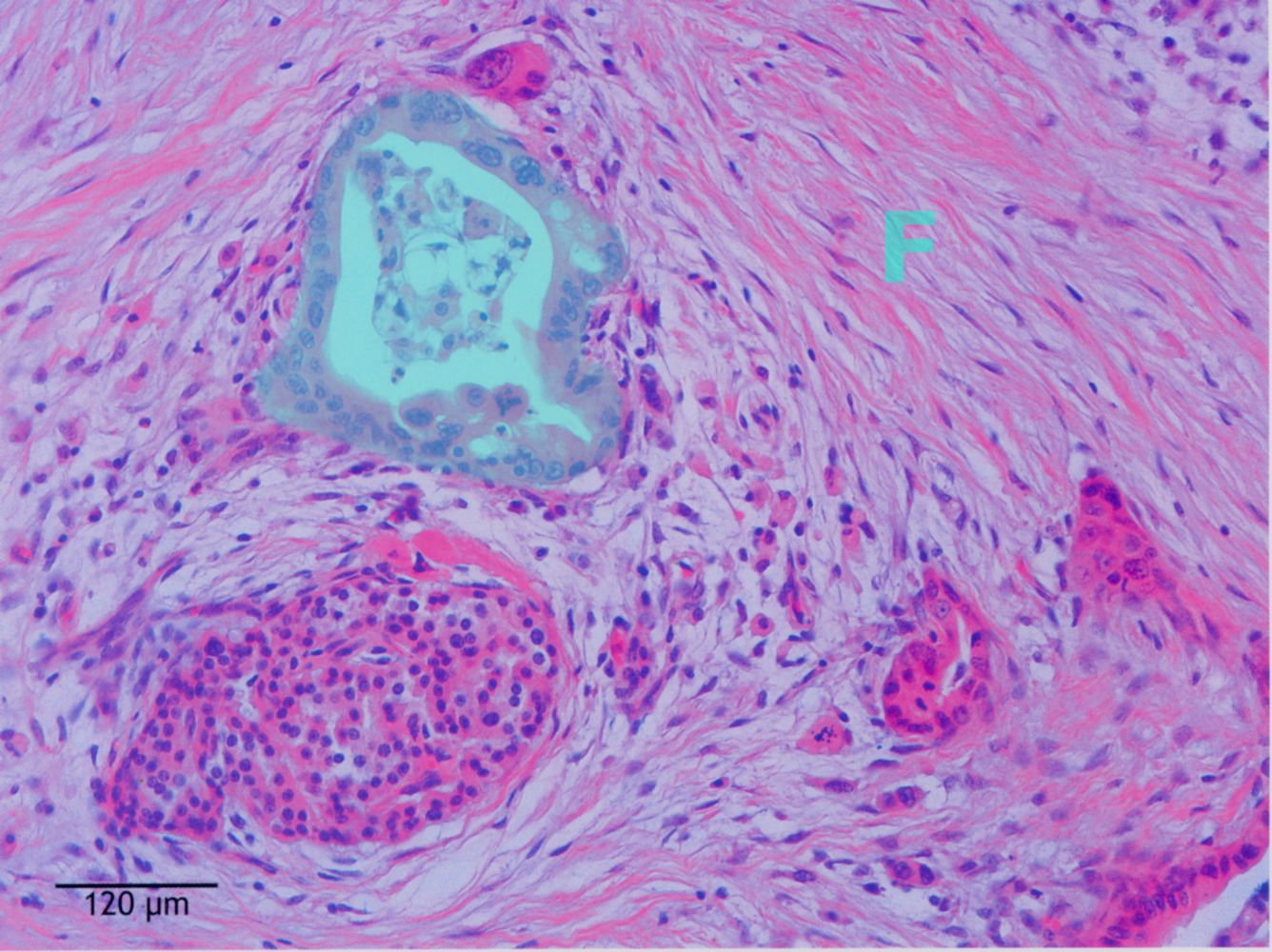
- Pancreatic exocrine tumors: originate from pancreatic acini and ducts
- Most common: ductal adenocarcinoma (95%)
- Altered ductal structures
- Cellular infiltration
- Adenocarcinoma of the pancreatic head is visible originating from the ductal cells, which have an atypical, uneven, multilayered epithelium (green overlay). F: fibrous septa
- Most common: ductal adenocarcinoma (95%)