Etiology
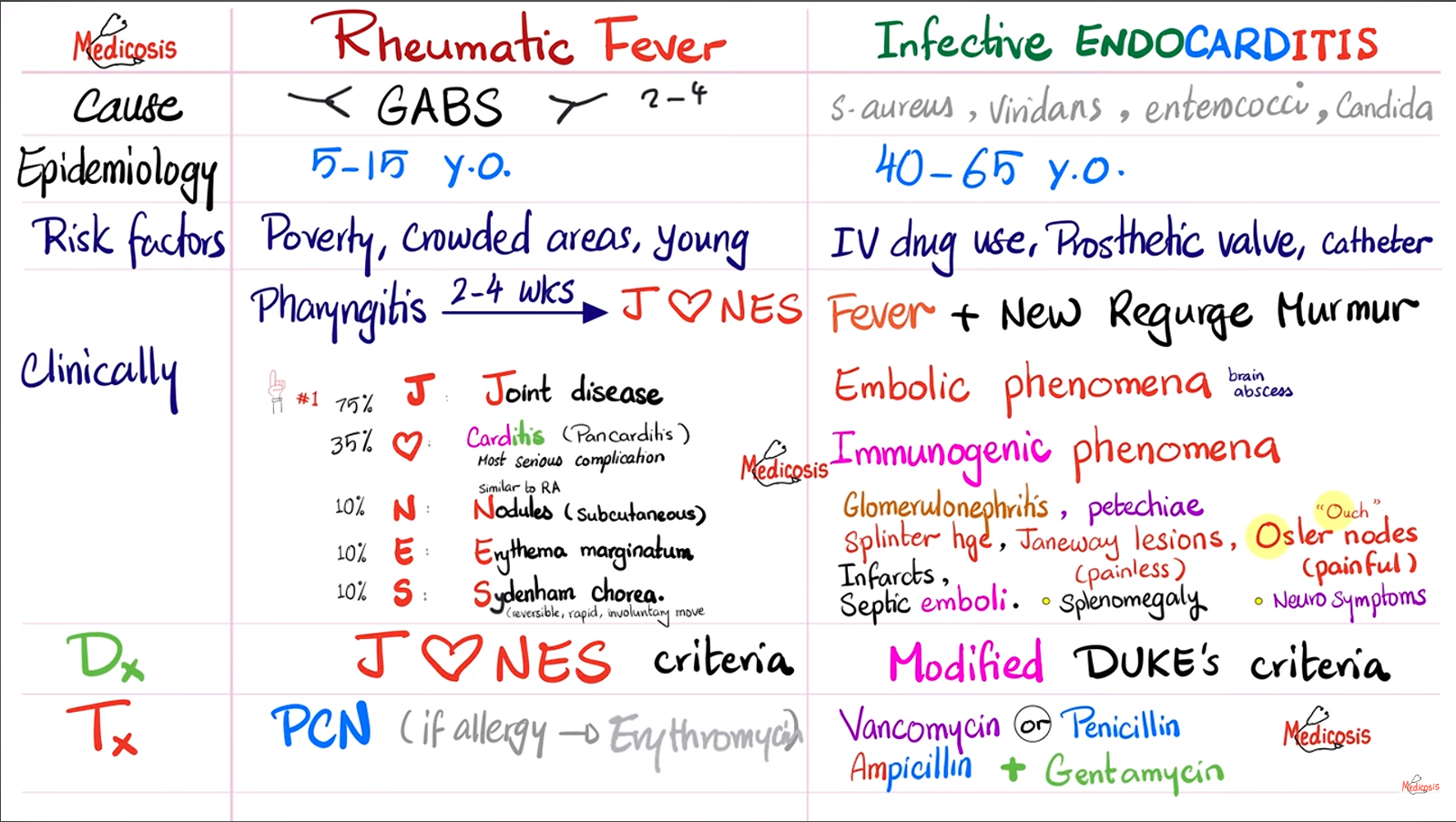
- Previous infection with group A β-hemolytic streptococcus (GAS), also referred to as Streptococcus pyogenes
- Usually acute tonsillitis or pharyngitis (“strep throat”)
- GAS infections of the skin (e.g., erysipelas, impetigo, cellulitis) tend to be complicated by poststreptococcal glomerulonephritis rather than rheumatic fever.
Pathophysiology
- Most commonly accepted mechanism involves the following: acute tonsillitis/pharyngitis caused by GAS without antibiotic treatment → development of antibodies against streptococcal M protein → cross-reaction of antibodies with nerve and myocardial proteins (most commonly myosins) due to molecular mimicry → type II hypersensitivity reaction → acute inflammatory sequela
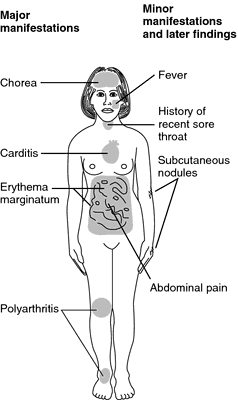
Clinical features
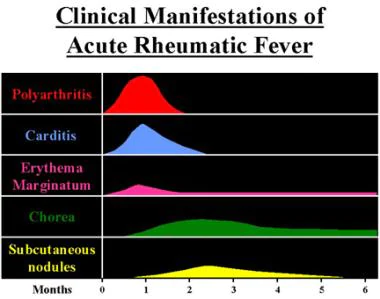
Clinical course
Need about 1 month to produce autoantibodies
- Heart
- Pancarditis (endocarditis, myocarditis, and pericarditis)
- Valvular lesions: most commonly on high-pressure valves
- Mitral valve (∼ 65% of cases)
- Early mitral regurgitation or prolapse
- Late mitral stenosis: Rheumatic fever is the most frequent cause of mitral stenosis.
- Mixed mitral stenosis/regurgitation
- Mitral valve (∼ 65% of cases)
- Aortic valve (∼ 25% of cases)
- CNS: Sydenham chorea (involuntary, irregular, nonrepetitive movements of the limbs, neck, head, and/or face)
- Occurs 1–8 months after the inciting infection
- In contrast to the other rheumatic manifestations, which usually occur within 3 weeks after initial infection.
- Pathophysiology: Streptococcal antigens lead to antibody production → antibodies cross-react with structures of the basal ganglia (particularly the striatum) and cortical structures → reversible dysfunction of cortical and striatal circuits
- Clinical features
- Sometimes asymmetrical or confined to one side (hemichorea)
- Additional motor symptoms (e.g., ballismus, muscle weakness) and speech disorders (slurred or “jerky” speech)
- Milkmaid grip: characterized by the inability to maintain muscle contraction in the hands → intermittent loss of contraction results in alternating squeeze and release of grip (“milking”)
- Choreic hand: characterized by intermittent wrist flexion with extension of the digits (“spooning” of the hand)
- Neuropsychiatric symptoms (e.g., inappropriate laughing/crying, agitation, anxiety, apathy, obsessive-compulsive behavior)
- Occurs 1–8 months after the inciting infection
- Skin
- Subcutaneous nodules
- Erythema marginatum: centrifugally expanding pink or light red rash with a well-defined outer border and central clearing.
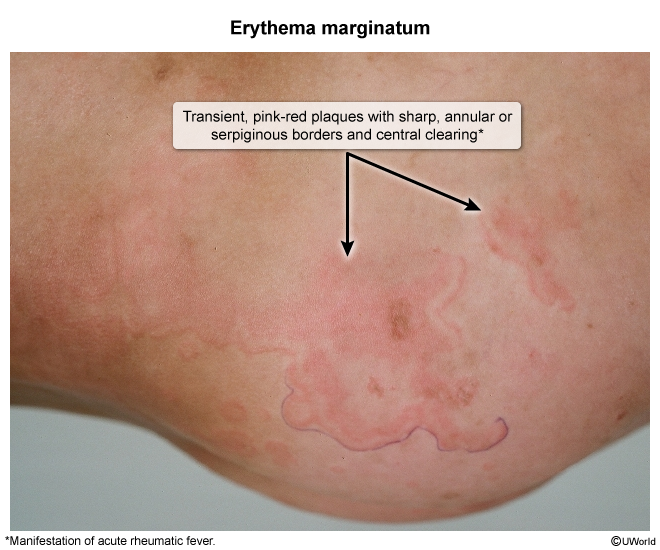
- Painless and nonpruritic
Diagnostics
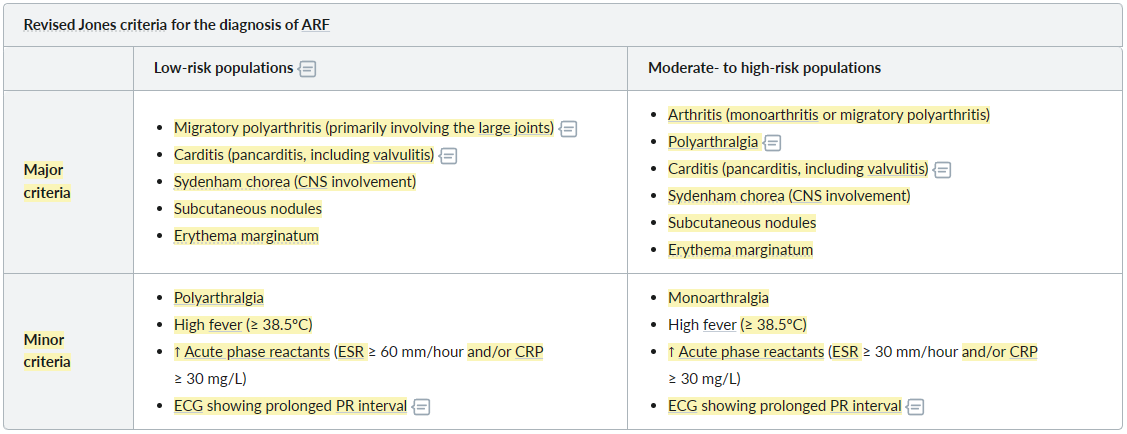
Revised Jones criteria
Mnemonic
- Major criteria: SPACE
- Subcutaneous nodules
- Pancarditis
- Arthritis (Polyarthritis; for moderate to high-risk population – monoarthritis also qualifies)
- Chorea
- Erythema marginatum
- Minor criteria: LEAF
- Long PR interval
- ESR ≥ 60mm/hr (or ≥ 30mm/hr in moderate to high-risk population) and CRP ≥ 3mg/dl
- Arthralgia (Polyarthralgia; for moderate to high-risk population – monoarthralgia also qualifies)
- Fever ( ≥ 38.5c; ≥ 38c for moderate to high-risk population )
ECG
- Most common: prolonged PR interval (first-degree AV block)
- Potential additional findings include:
- Second-degree AV block
- Complete heart block
- Sinus tachycardia
- Accelerated junctional rhythm
- ECG features of pericarditis
Tip
Whenever you see marked left atrial abnormality or atrial fibrillation in the presence of right ventricular hypertrophy signs, always think about rheumatic mitral valve disease. Mitral stenosis is the only single lesion that can readily account for the combination of left atrial enlargement and right ventricular hypertrophy.
Pathology
- Myocardial findings
- Aschoff bodies
- Granuloma of rheumatic inflammation
- Central area of fibrinoid necrosis
- Surrounded by characteristic multinucleated giant cells (Aschoff cells) and other inflammatory cells (mononuclear cells, plasma cells, and T lymphocytes) due to a type IV hypersensitivity reaction.
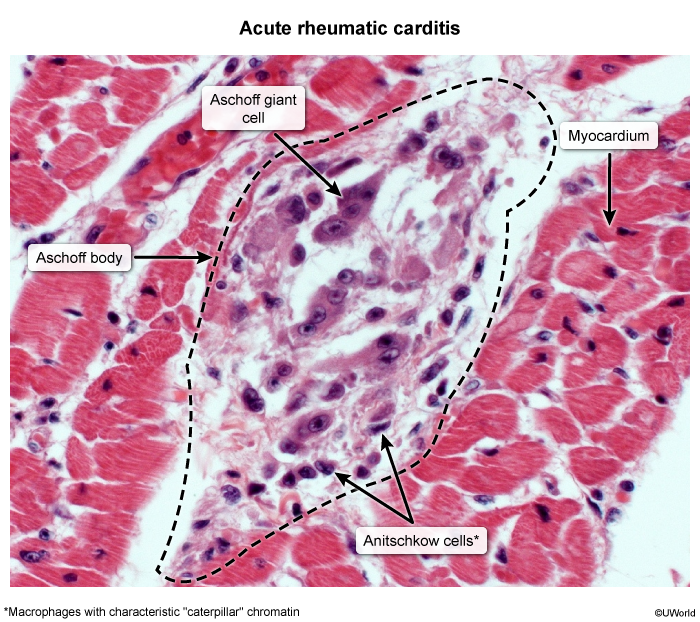
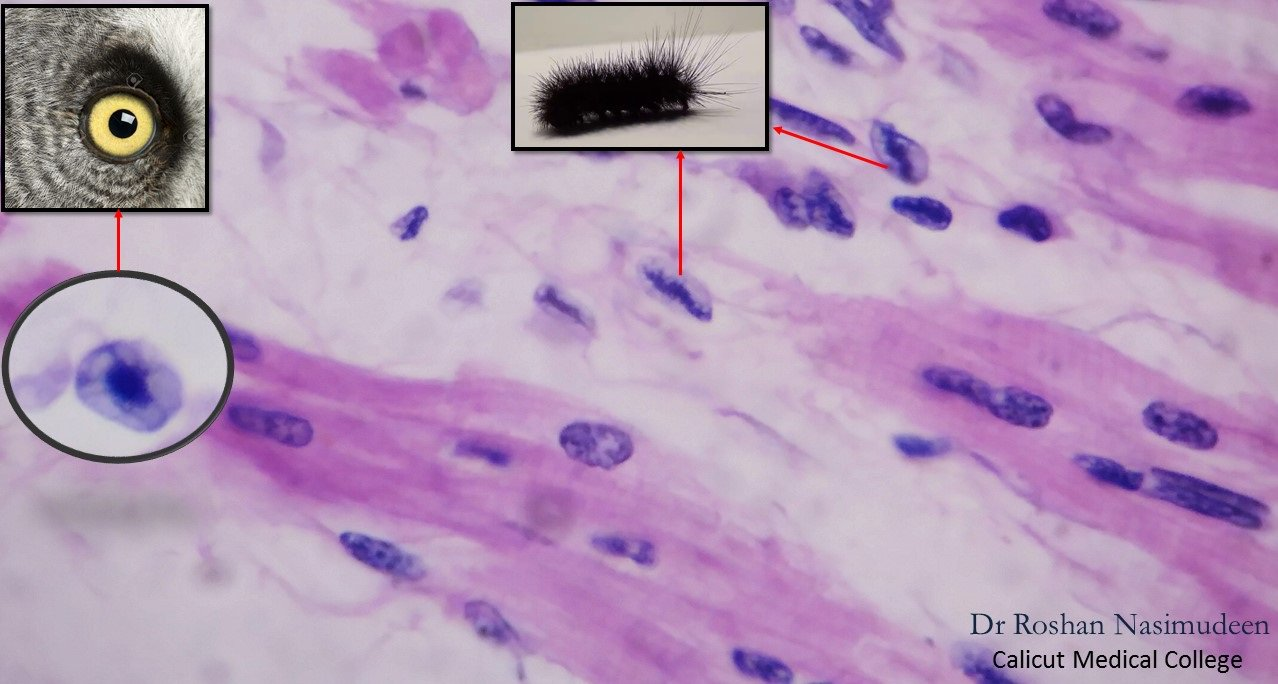
- Anitschkow cells
- Cardiac histiocytes (mononuclear cells) appearing in Aschoff bodies
- Large and elongated cells
- Longitudinal section: ovoid nucleus containing wavy, caterpillar-like bar of chromatin (caterpillar cell)
- Transverse section: owl-eye appearance
- Aschoff bodies