Trauma, e.g., deceleration injury in a motor vehicle collision, or iatrogenic injury during valve replacements or graft surgery (traumatic aortic dissection)
Progressive weakening of arterial wall due to elastin degradation and inflammation; atherosclerosis leads to oxidative stress and matrix metalloproteinase activation
Intimal tear allows blood to enter media, creating false lumen; can be triggered by hypertensive crisis or inherited connective tissue disorders
Onset
Gradual
Sudden, acute
Pain
Usually asymptomatic; may have dull abdominal/back pain
Severe, tearing chest/back pain; migrating
Physical Exam
Pulsatile abdominal mass
Unequal pulses, BP differences between arms
Complications
Rupture with hemorrhagic shock
Organ ischemia, tamponade, aortic rupture
Imaging
Ultrasound, CT with contrast
CT angiogram, TEE
Treatment
Endovascular repair (EVAR) or open surgery if >5.5cm
Emergency surgery (Type A), medical management (Type B)
Mortality
80% if ruptured; 5% with elective repair
50% at 48h without treatment (Type A)
Clinical features
Diagnostics
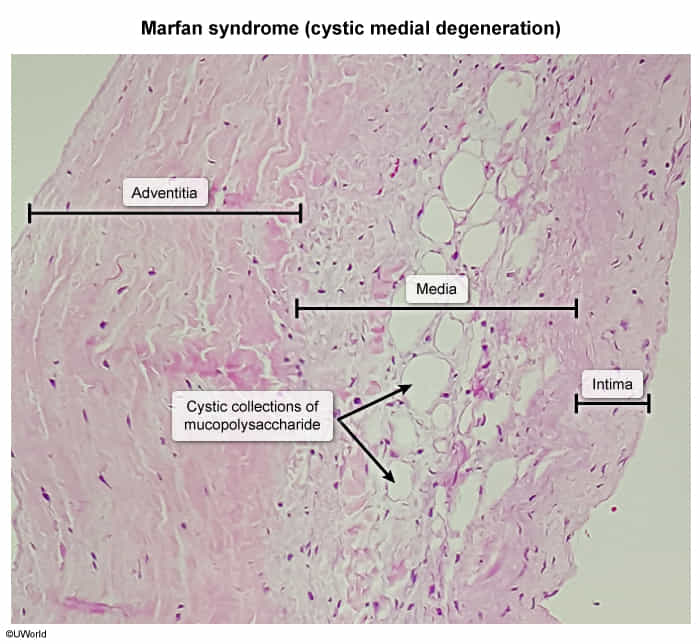
Pathology
Cystic medial degeneration: a degeneration (necrosis) of large blood vessels such as the aorta.