Etiology
- Premature birth
- Maternal diabetes mellitus: leads to ↑ fetal insulin, which inhibits surfactant synthesis
- Hereditary
- Cesarean delivery: results in lower levels of fetal glucocorticoids than vaginal delivery, in which higher levels are released as a response to stress from uterine contractions
- Hydrops fetalis
- Multifetal pregnancies
- Male sex
Pathophysiology
- Deficiency of pulmonary surfactant in premature infants.
- Surfactant is produced by Type II pneumocytes starting around 24-28 weeks gestation, with mature levels achieved after 35 weeks.
- Key component of surfactant: Dipalmitoylphosphatidylcholine (DPPC).
- Function of surfactant: ↓ alveolar surface tension, which prevents atelectasis at end-expiration.
- Deficiency → ↑ alveolar surface tension → widespread atelectasis → ↓ lung compliance → V/Q mismatch → hypoxemia & hypercapnia. t
Clinical features
- Maternal history of premature birth
- Onset of symptoms: usually immediately after birth but can occur up to 72 hours postpartum
- Signs of increased respiratory effort
- Tachypnea
- Nasal flaring and moderate to severe subcostal/intercostal and jugular retractions
- Characteristic expiratory grunting
- Decreased breath sounds on auscultation
- Cyanosis due to pulmonary hypoxic vasoconstriction
Diagnostics
- X-ray chest
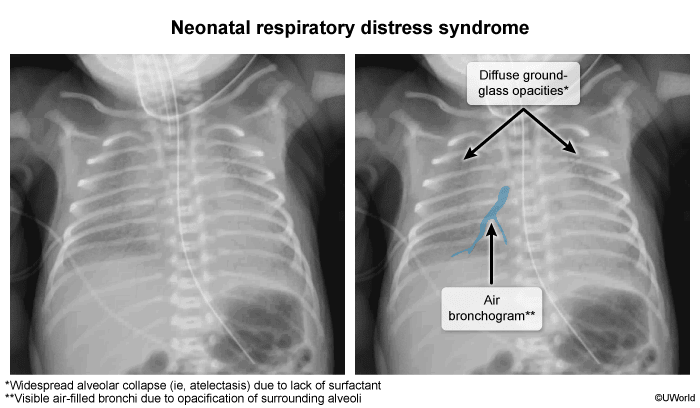
- Interstitial pulmonary edema with perihilar streaking
- Diffuse, fine, reticulogranular (ground-glass) densities with low lung volumes and air bronchograms
- Atelectasis
- Prenatal Assessment: Lecithin-to-sphingomyelin (L/S) ratio in amniotic fluid.
- L/S ratio < 2.0 indicates lung immaturity.
- Presence of phosphatidylglycerol signifies lung maturity.
- The amount of lecithin, which is the major component of surfactant, starts increasing after week 26 of gestation.
- The lower the lecithin-sphingomyelin ratio, the more likely it is that the lungs are immature.
Differential diagnostics
Apnea of prematurity
- Etiology/Pathophysiology
- Common in preterm infants (<37 weeks gestation) due to immature respiratory control centers.
- Incidence inversely proportional to gestational age.
- Types: Central (immature brainstem drive), Obstructive (airway collapse), Mixed (most common).
- Clinical Features & Diagnostics
- Defined as respiratory pause >20 seconds OR shorter pause with bradycardia (<100 bpm) or desaturation (<85%).
- Onset typically 2-3 days post-birth.
- Diagnosis of exclusion (rule out sepsis, metabolic, CNS, cardiac issues).
- Car Seat Challenge before discharge.
- Treatment
- Tactile stimulation, proper positioning.
- Pharmacologic: Methylxanthines (e.g., Caffeine citrate - preferred for central stimulation).
- Respiratory Support: Nasal CPAP (for obstructive/mixed apnea), mechanical ventilation for severe cases.
- Prognosis
- Excellent; resolves as infant matures, typically by 40-44 weeks postmenstrual age.
Meconium Aspiration Syndrome (MAS)
-
Epidemiology & Risk Factors
- Term / post-term infants (rarely < 37 wks).
- Fetal hypoxia/distress (triggers in utero meconium passage).
-
Clinical Features
- Meconium-stained amniotic fluid; green/yellow stained vernix.
- Immediate resp distress (tachypnea, grunting, retractions).
- Barrel chest (ball-valve air trapping).
-
Diagnosis
- Initial/Screening: CXR (shows patchy, bilateral infiltrates + hyperinflation/flattened diaphragms).
- Confirmatory/Key Tests: Clinical dx; ABG (hypoxemia); Echo (to r/o secondary PPHN).
-
Differential Diagnostics
- TTN: C-section, CXR shows fluid in fissures/normal vols; resolves rapidly.
- RDS: Preterm, CXR shows ground-glass opacities/low lung vols.
- Neonatal PNA: Prolonged ROM/GBS+; CXR looks identical to MAS.
-
Management
- Resuscitation (NRP):
- Vigorous: Routine care.
- Non-vigorous: Positive Pressure Ventilation (PPV). (High-Yield: Routine intubation/suction is NO LONGER recommended).
- Supportive: O2, CPAP, or mech vent.
- Medical Therapy: Empiric Abx (Amp + Gent) + exogenous surfactant.
- Refractory/PPHN: Inhaled NO (iNO) → ECMO.
- Resuscitation (NRP):
-
Complications
- Persistent Pulmonary HTN of Newborn (PPHN). c
- Air leaks (Pneumothorax).
- Hypoxic-ischemic encephalopathy (HIE).
Persistent pulmonary hypertension of the newborn (PPHN)
-
Epidemiology & Risk Factors
- Term/post-term neonates.
- Meconium Aspiration Syndrome (MAS) (classic), perinatal asphyxia, CDH, maternal SSRI/NSAID use in 3rd trimester.
-
Clinical Features
- Severe cyanosis & resp distress <24h of life.
- High PVR → R→L shunt across PDA/PFO.
- PE: Prominent RV impulse, loud single P2, harsh systolic murmur (TR).
-
Diagnosis
- Initial: Pre/Post-ductal SpO2 gradient (>5-10% difference between R arm & leg).
- Screening: Failed Hyperoxia Test (PaO2 does not improve on 100% O2, indicating fixed R→L shunt).
- Confirmatory: Echocardiogram (shows ↑ RV pressure, R→L shunting; r/o structural CHD).
-
Differential Diagnostics
- Cyanotic CHD (e.g., TGA): Structural defects visible on Echo.
- RDS: Premature infant; CXR shows ground-glass opacities/air bronchograms.
-
Management
- Supportive: O2, mechanical ventilation (correct hypoxia/acidosis).
- Targeted Therapy: Inhaled Nitric Oxide (iNO). Acts as a selective pulmonary vasodilator without causing systemic hypotension. c
- Refractory: ECMO.
-
Complications
- Sensorineural hearing loss (due to prolonged hypoxia & ototoxic Abx).
- Neurodevelopmental delay.
Complications
Bronchopulmonary dysplasia (BPD)
- Definition: chronic lung condition secondary to prolonged mechanical ventilation and oxygen therapy for NRDS
- Etiology: Pulmonary barotrauma and oxygen toxicity with subsequent inflammation of lung tissue due to ventilation of the immature lung (ventilation for more than 28 days)
- Clinical features
- Seen in infants < 32 weeks
- Persistence of symptoms similar to NRDS (e.g., tachypnea, grunting, nasal flaring)
- Episodes of desaturation
- Diagnostics
- X-ray chest: diffuse, fine, granular densities, areas of atelectasis interspersed with areas of hyperinflation
- Blood gas analysis: respiratory and metabolic acidosis
- Histology: atelectasis, fibrosis, emphysematous alveolar changes (decreased number and septation of alveoli)
- Treatment: controlled oxygenation, diuretics, rarely glucocorticoids