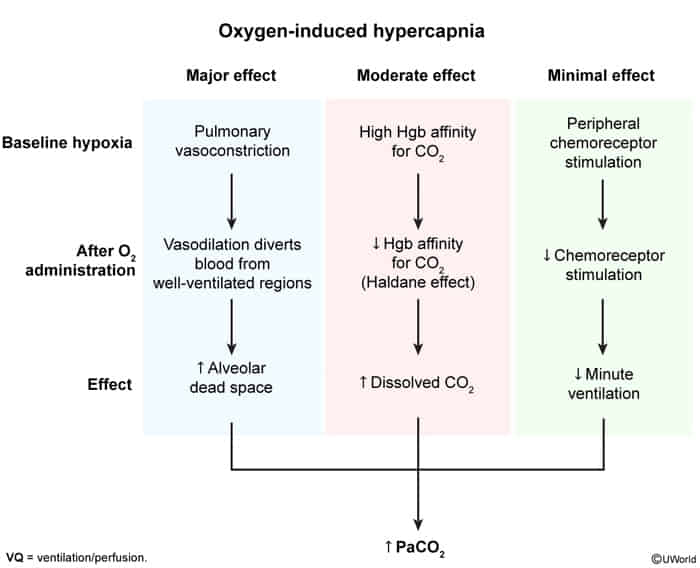
Haldane effect: ↑ FiO2 → ↑ oxygenated Hb, which has a reduced affinity to bind CO2 (right shift in the CO2 dissociation curve) → CO2 being released from Hb and RBCs → ↑ PaCO2
Risk factors
Any patient with risk factors for hypercapnic respiratory failure who is receiving supplemental oxygen
PaO2 is > 75 mm Hg
Acute illness or new oxygen therapy in patients with chronic hypercapnic respiratory failure
Management
Gradually titrate oxygen back to 88–92%.
Noninvasive ventilation in patients with decompensated hypercapnic respiratory failure who are within target saturations.
Prevention
Close monitoring for symptoms of hypercapnia.
Patients at risk of hypercapnic respiratory failure: ABGs should be performed if drowsiness or other symptoms of hypercapnia develop, if saturations deteriorate, or if acute breathlessness occurs.