Mechanism: a sudden and severe rise in the esophageal intraluminal pressure results in tearing of the esophageal mucous membrane, as well as the submucosal arteries and veins
typically follows a period of severe, bloodless vomiting
Possible shock
Diagnostics
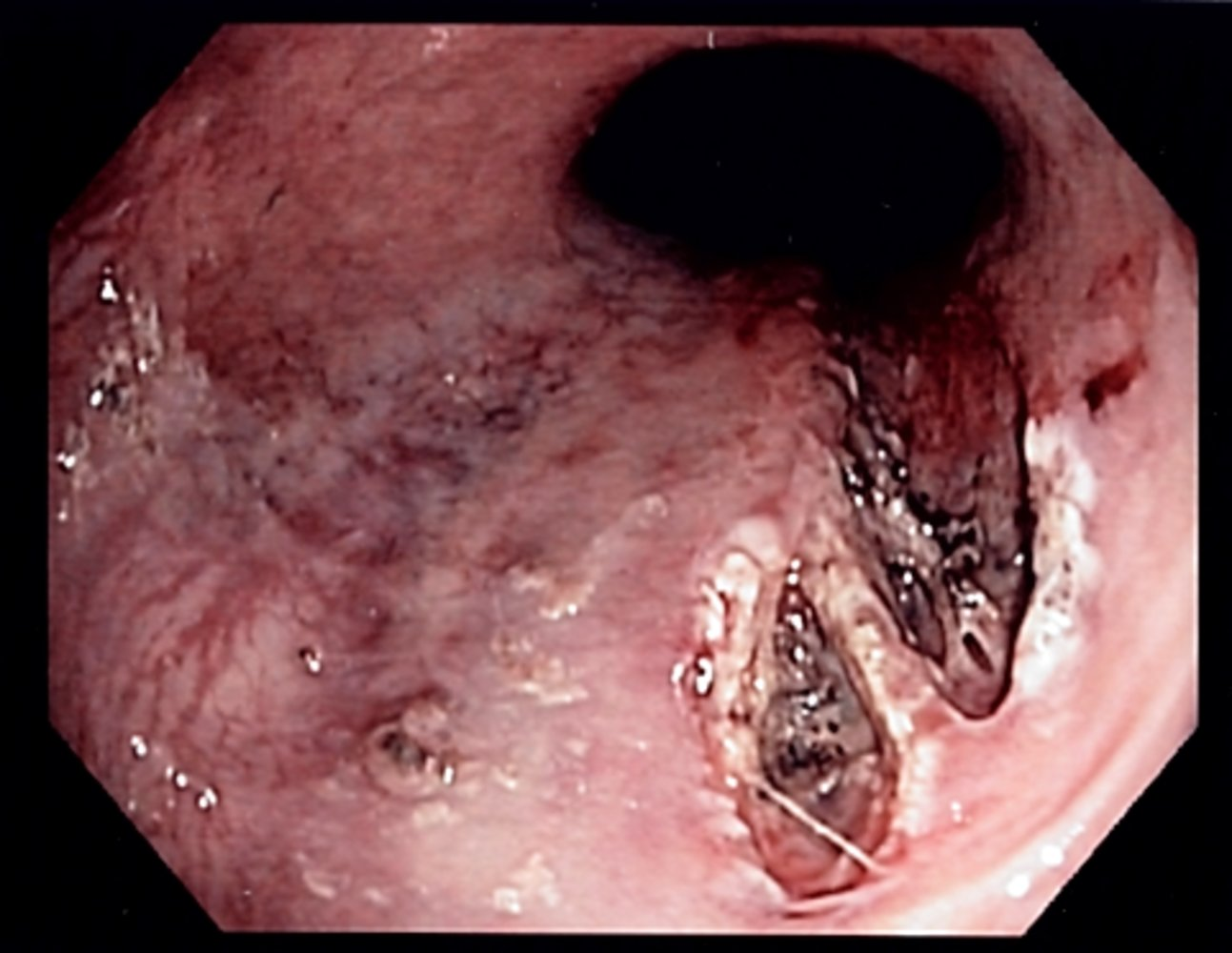
EGD
Typical findings
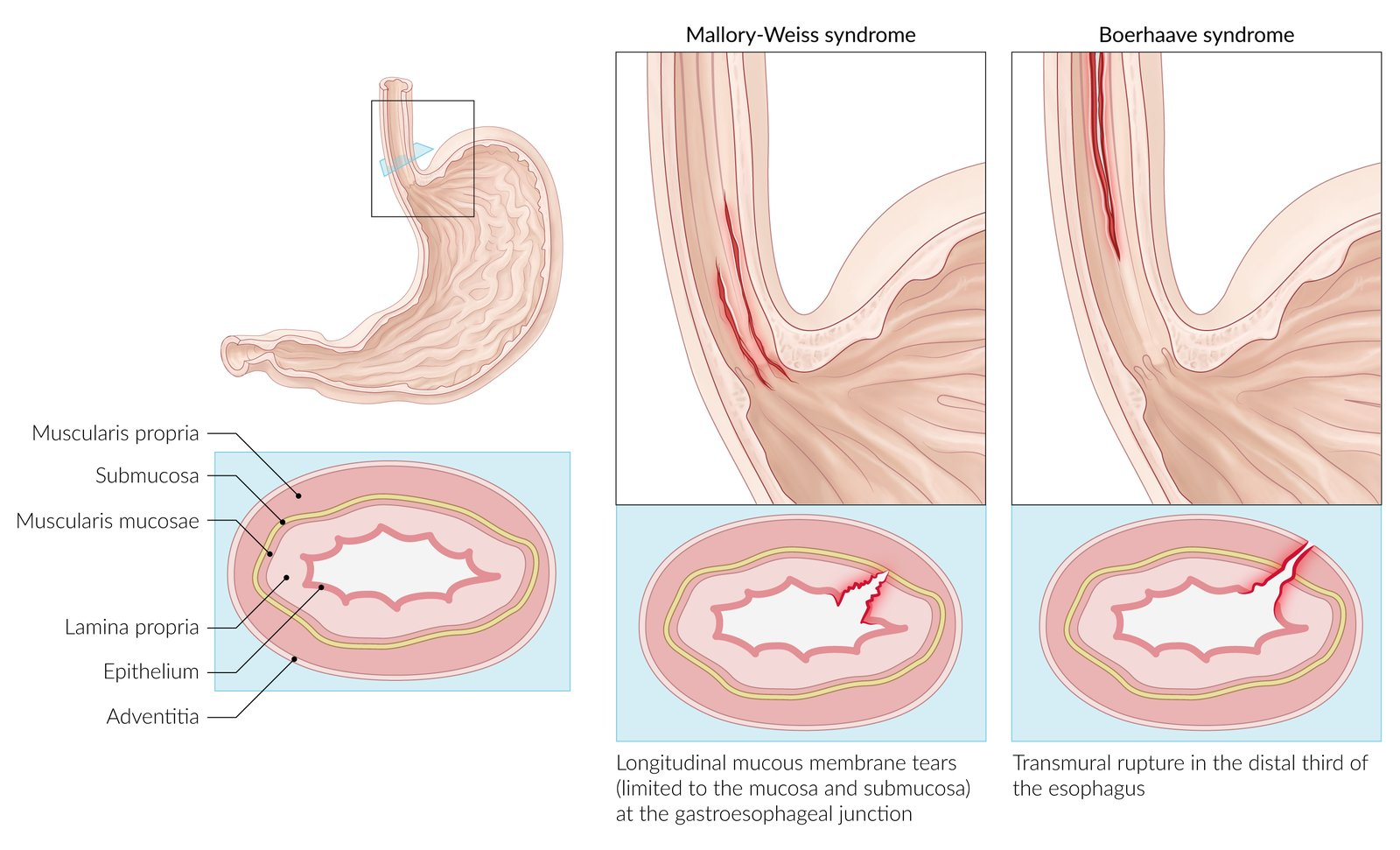
Often a single longitudinal tear (but multiple tears are possible) in the mucosa at the gastroesophageal junction or in the cardia of the stomach which are limited to the mucosa and submucosa
A fibrin crust over the split, a clot, or active bleeding may be evident.
Differential diagnostics
Characteristics of Gastroesophageal Mural Injury
Mallory-Weiss Syndrome
Boerhaave Syndrome
Etiology
Forceful retching
Forceful retching
Mucosal tear
Transmural tear
Submucosal venous or arterial plexus bleeding
Spillage of esophageal air/fluid into surrounding tissues