Epidemiology
- HFrEF (LVEF ≤40%): CAD/prior MI (most common), dilated cardiomyopathy (ETOH, viral, cocaine, Chagas), valvular disease (chronic AR/MR).
- HFpEF (LVEF ≥50%): HTN (most common - causes LVH), restrictive cardiomyopathy (amyloidosis, sarcoidosis), obesity, advanced age. c
- Adiposity induces a systemic proinflammatory state → coronary microvascular endothelial inflammation → cardiomyocyte stiffness and interstitial fibrosis.
- General RFs: DM2, Smoking, OSA, CKD.
Etiology
Pathophysiology
- Pressure Overload (e.g., chronic hypertension, aortic stenosis) → Concentric Hypertrophy (sarcomeres in parallel) → initially HFpEF → decompensates to HFrEF.
- Volume Overload (e.g., aortic/mitral regurgitation, Ischemic Cardiomyopathy) → Eccentric Hypertrophy (sarcomeres in series) → HFrEF.
Clinical features
- Left-sided (Congestion): Dyspnea on exertion (DOE), orthopnea, paroxysmal nocturnal dyspnea (PND), displaced PMI, S3 gallop (ventricular filling into dilated/compliant LV; specific for HFrEF), bibasilar crackles.
- Paroxysmal nocturnal dyspnea: Patients with PND wake up acutely short of breath and typically need to sit upright at the edge of the bed for 10-20 minutes for relief
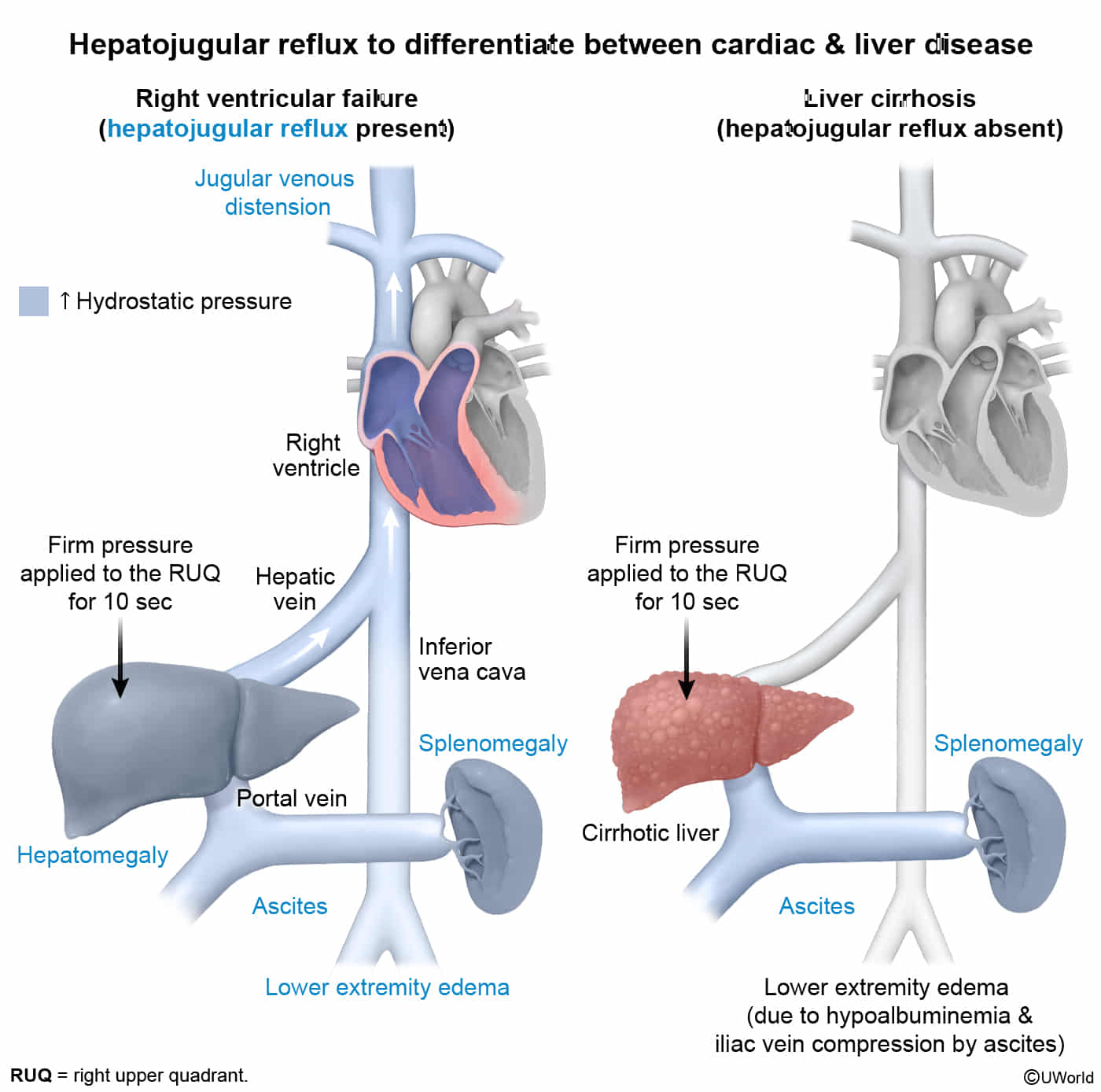
- Right-sided (Venous HTN): Peripheral edema, JVD, hepatojugular reflux, congestive hepatomegaly (nutmeg liver), S4 gallop (atrial kick against stiff LV; typical of HFpEF/HTN).
- Hepatojugular reflux is useful for differentiating between cardiac disease– and liver disease–related causes of ascites, splenomegaly, and lower extremity edema.
- Hepatojugular reflux is useful for differentiating between cardiac disease– and liver disease–related causes of ascites, splenomegaly, and lower extremity edema.
Diagnostics
Pathology
- Sputum analysis in patients with pulmonary edema may show heart failure cells (hemosiderin-containing cells).
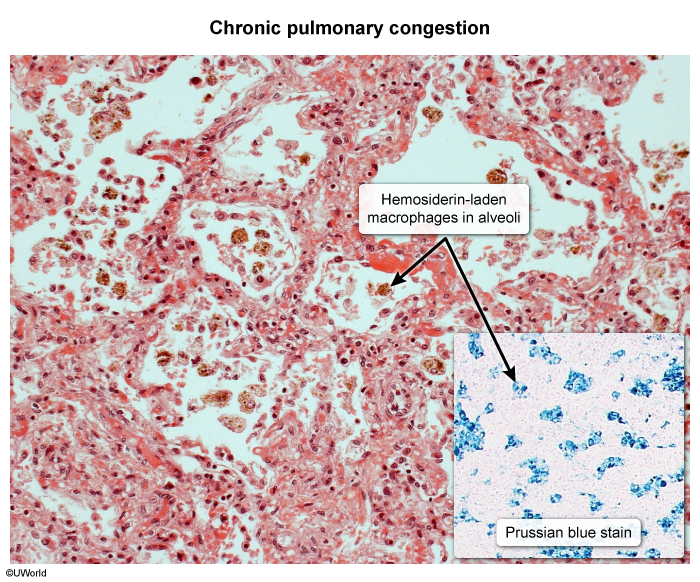
- Pulmonary venous congestion may result in intra-alveolar bleeding. Macrophages that subsequently phagocytose the erythrocytes are called “heart failure cells.” These cells may also be detected in the sputum of patients with pulmonary infarction, vasculitis, or aspiration of blood.
- Their color is most likely due to hemosiderin from ingested erythrocytes.
ECG
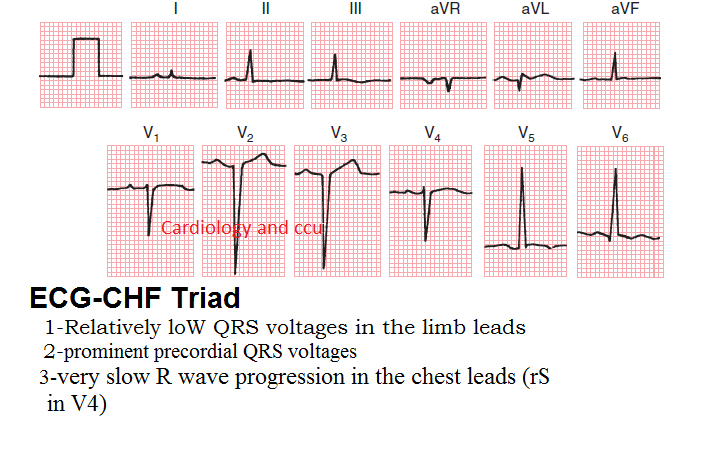
- ECG-CHF triad
- Low QRS voltages in the limb leads (caused by peripheral edema in CHF patients)
- Left ventricular hypertrophy (prominent precordial QRS voltages)
- Very slow R wave progression in chest leads (rS in V4)
Additional laboratory studies
- CBC (rule out anemia), CMP (evaluate hyponatremia indicating severe HF, BUN/Cr for cardiorenal syndrome, LFTs for congestive hepatopathy).
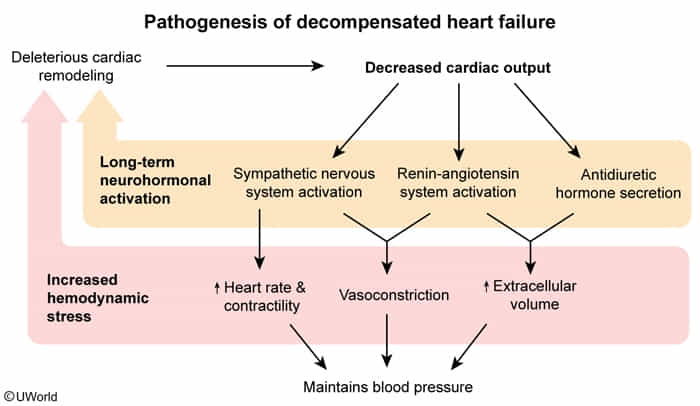
- Low CO triggers massive, non-osmotic release of ADH (vasopressin) + ↑ RAAS → Kidneys retain free H2O in excess of Na+ → Dilutional Hyponatremia.
- Serum Na+ level directly reflects the severity of neurohormonal activation. It is a major independent predictor of mortality/poor prognosis in HF. c
Treatment
| Agent | Mortality Benefit |
|---|---|
| Angiotensin receptor-neprilysin inhibitor (e.g., sacubitril-valsartan) OR ACE inhibitor (e.g., lisinopril) OR Angiotensin II receptor blocker (e.g., losartan) | Yes |
| Beta blocker (e.g., metoprolol, carvedilol) | Yes |
| Mineralocorticoid receptor antagonist (e.g., spironolactone, eplerenone) | Yes |
| Sodium-glucose cotransporter-2 inhibitor (e.g., dapagliflozin, empagliflozin) | Yes |
| Diuretic (e.g., furosemide, metolazone) | No, only improves symptoms & reduces hospitalization. |
| Digoxin | No, only reduces hospitalization. |
Explanation
The primary role of MRAs (Spironolactone, Eplerenone) in HFrEF is neurohormonal blockade, not diuresis. c
- Primary Mechanism (Mortality Benefit):
- In heart failure, the renin-angiotensin-aldosterone system (RAAS) is chronically activated.
- Persistently high aldosterone levels are directly harmful to the heart, causing:
- Myocardial Fibrosis: Promotes collagen deposition, leading to stiffening of the ventricle.
- Adverse Cardiac Remodeling: Contributes to the progressive enlargement and dysfunction of the heart.
- Endothelial Dysfunction & Inflammation: Worsens vascular health.
- MRAs directly block the aldosterone receptor, preventing these cardiotoxic effects. This slows disease progression and improves survival.
- Secondary Mechanism (Diuresis):
- MRAs have a mild diuretic effect by promoting sodium/water excretion and potassium retention in the collecting ducts.
- This effect is weak and is not the reason they are a cornerstone of therapy.
HFrEF (EF ≤40%): Chronic Management
- Goal: Mortality reduction via “Quadruple Therapy” or the “4 Pillars”.
- 1. ARNI (Sacubitril/Valsartan): Preferred over ACEi/ARB. A 36-hour washout period is required when switching from an ACE inhibitor.
- 2. β-Blockers: Only use evidence-based ones (Carvedilol, Metoprolol Succinate, Bisoprolol). Do not start or increase during acute decompensation.
- 3. MRAs (Spironolactone, Eplerenone): Block aldosterone-mediated fibrosis. Monitor for hyperkalemia.
- 4. SGLT2 Inhibitors (-flozins): Reduce mortality and hospitalizations, even in non-diabetics.
- Symptom & Add-On Therapy:
- Loop Diuretics (e.g., Furosemide): For congestion relief (dyspnea, edema). No mortality benefit.
- Hydralazine + Isosorbide Dinitrate: Provides mortality benefit in African American patients (NYHA III-IV) on optimal therapy, or as an alternative for those intolerant to ACEi/ARB/ARNI.
- MOA: Hydralazine (arterial vasodilator) reduces afterload; Isosorbide dinitrate (venodilator) reduces preload.
- Ivabradine: Reduces hospitalizations. Use in stable patients on max βB dose with sinus rhythm & HR ≥70 bpm.
- MOA: Selectively inhibits the If (“funny”) current in the SA node to slow heart rate.
HFpEF (EF ≥50%): Chronic Management
- Goal: Control symptoms and comorbidities (especially HTN).
- Key Therapies:
- SGLT2 Inhibitors (-flozins): Proven to reduce HF hospitalizations.
- Diuretics: For fluid overload symptoms.
- Manage comorbidities aggressively (HTN, AFib, obesity, diabetes).
Acute Decompensated HF (ADHF)
- Goal: Relieve congestion (“wet”) and improve perfusion (“warm”).
- Mnemonic “LMNOP” for initial management:
- Lasix (IV Loop Diuretics): Mainstay for volume removal.
- Morphine: Historically used for anxiolysis and venodilation (rarely used now).
- Nitrates (e.g., Nitroglycerin): IV vasodilators to reduce preload and afterload if BP is adequate.
- Oxygen: If patient is hypoxic (SpO2 <90%).
- Position: Have the patient sit upright to decrease venous return.
- “Warm & Wet” (Congested but well-perfused):
- Tx: IV Loop Diuretics + IV Vasodilators (Nitroglycerin).
- “Cold & Wet” (Congested and poorly perfused/hypotensive):
- Tx: IV Loop Diuretics + Inotropes (Dobutamine, Milrinone) to improve cardiac output. May require vasopressors if in shock.
Drugs
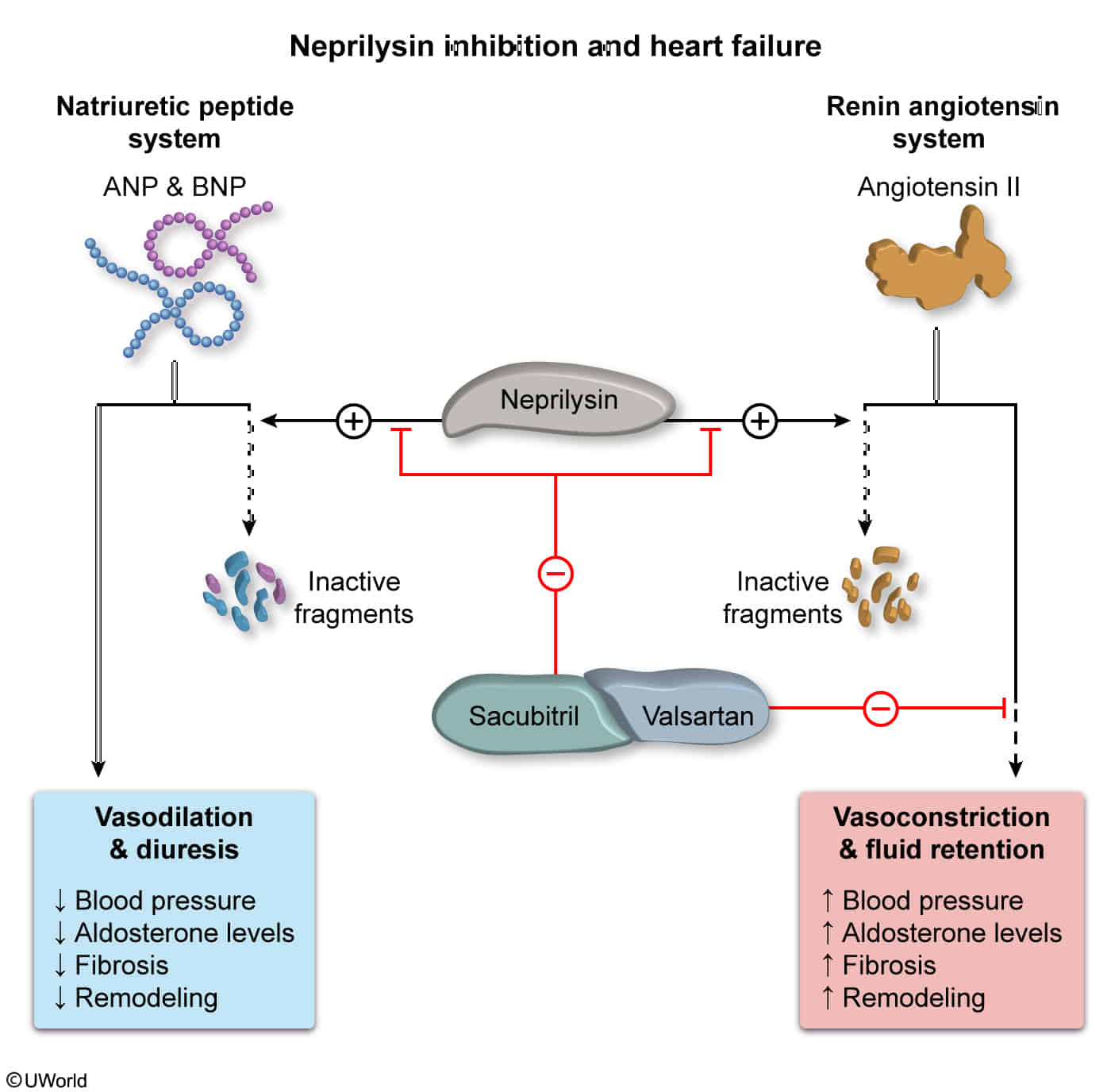
Angiotensin receptor-neprilysin inhibitors (ARNIs)
- Drug names: sacubitril/valsartan
- Sacubitril: Inhibits neprilysin (a neutral endopeptidase) prevents degradation of natriuretic peptides (ANP, BNP), bradykinin, and substance P promotes vasodilation, natriuresis, diuresis, and cardiac remodeling/fibrosis.
- Valsartan: Angiotensin II Receptor Blocker (ARB). Crucial addition because neprilysin inhibition alone reflexively upregulates the RAAS pathway. Blocking the AT1 receptor mitigates this effect.
- Indication: Stage C or D HFrEF (preferred initial agent for RAAS inhibition)
- High-Yield Administration Rules (Step 2 CK Focus)
- The 36-Hour Washout: When switching a pt from an ACEi to an ARNI, there MUST be a 36-hour washout period. Taking both massive in bradykinin life-threatening angioedema.
- ARB Transition: No washout period is required when switching from an ARB to an ARNI.
- Adverse Effects & Complications
- Hypotension: Most common dose-limiting side effect.
- Angioedema: Increased risk compared to ARB alone. Absolute contraindication if pt has a hx of hereditary angioedema or ACEi-induced angioedema.
- Hyperkalemia: Due to RAAS blockade ( aldosterone).
- Renal Impairment: Transient Cr (similar to ACEi/ARBs; monitor closely).
- Teratogenicity: Contraindicated in pregnancy (fetal renal toxicity).
Complications
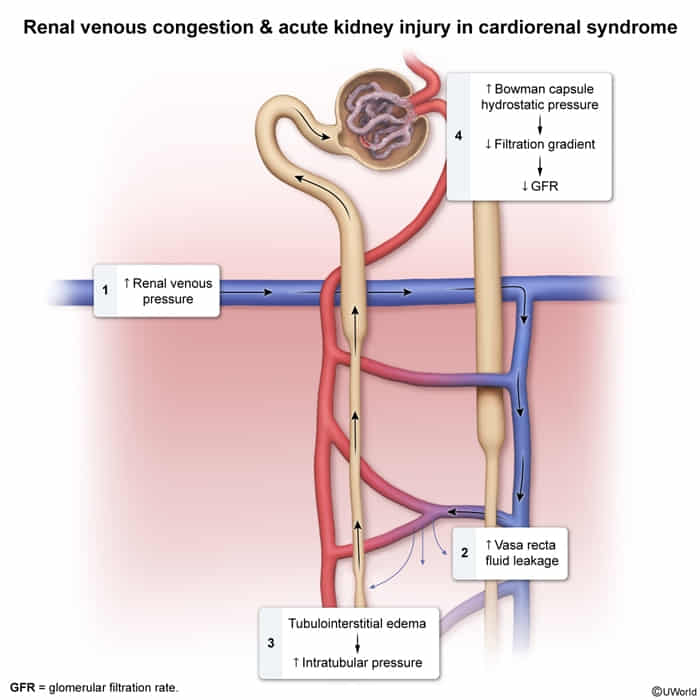
Cardiorenal syndrome
- Definition: Acute Decompensated Heart Failure (ADHF) causing Prerenal AKI, primarily driven by Renal Venous Congestion (high afterload on the kidney). c
- Key Labs: BUN/Cr > 20:1, FeNa < 1%, Urine Na < 20 mEq/L (indicates avid Na/Water retention).
- Best Initial Test: Transthoracic Echo (TTE) to assess pump function.
- First-Line Management: IV Loop Diuretics (Furosemide). Goal is to decongest the kidney. c
- Refractory Management: Add Metolazone (Thiazide) for sequential blockade.
- Unstable/Hypotensive Management: Start Inotropes (Dobutamine) to restore perfusion before diuresis.
- Critical Exam Rule: Do not stop diuresis for mild Creatinine bumps if the patient is still volume overloaded (wet).
- Contraindications: NSAIDs (worsens vasoconstriction). Stop ACEi/ARB temporarily if Hyperkalemia or severe AKI develops.