Epidemiology
Bimodal age distribution; mostly affects children (between the ages of 3–12 years) and patients > 60 years of age
Etiology
- Prior infection with group A beta-hemolytic streptococci (GAS, S pyogenes)
- In children
- Infection of the mouth and pharynx (tonsillitis, pharyngitis): PSGN typically arises 1–2 weeks following infection.
- Soft tissue infections (erysipelas, impetigo): PSGN typically arises 4–6 weeks following infection.
- In children
Pathophysiology
Infection with nephritogenic strains of group A beta-hemolytic streptococci → streptococcal antigen deposit within the glomerular basement membrane → immune complexes formation (Type III hypersensitivity reaction) → complement activation (↑ consumption of complement factors) → destruction of the glomeruli → immune complex-mediated glomerulonephritis and nephritic syndrome
Clinical features
Approx. 50% of patients remain asymptomatic. Symptoms occur approximately 1–6 weeks following an acute infection.
- Nephritic syndrome
- Hematuria: tea- or cola-colored urine
- Hypertension: can lead to headaches
- Edema (prominent facial edema)
- Oliguria
- Influenza-like symptoms
- Flank pain
Diagnostics
Initial evaluation
- Urinalysis with microscopy: nephritic sediment
- C3 complement, C4 complement levels: classically shows ↓ C3 complement with normal C4 complement
Tip
If both C3 and C4 complement levels are decreased, consider other causes of glomerulonephritis with low serum complement levels and possible nonrenal causes of low complement levels (e.g., liver failure, nonrenal protein-losing conditions).
Evidence of preceding GAS infection
- Antistreptococcal antibody titers
- Findings: ↑ ASO, ↑ anti-DNase B antibodies
- Isolation of group A beta-hemolytic streptococci
- Pharyngitis: rapid strep test, throat culture
- Skin lesions: wound cultures
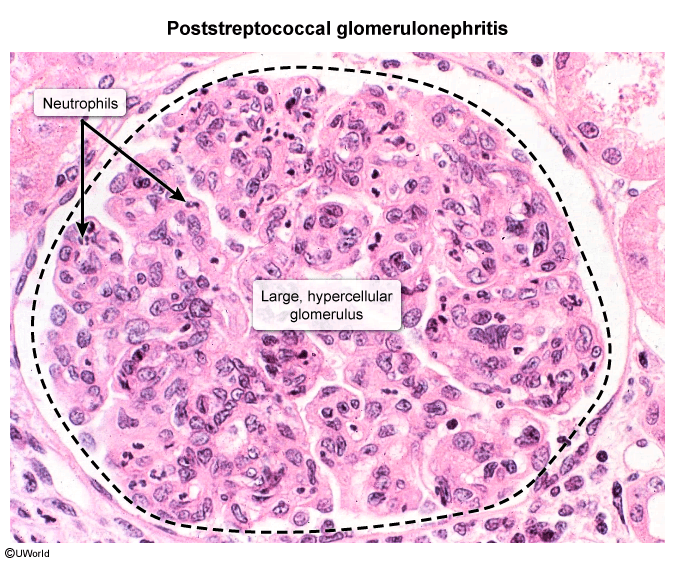
Microscopy
- LM: hypercellular glomeruli
Treatment
Prognosis
Increased age is the most important poor prognostic factor
- Recovery usually occurs within 6–8 weeks.
- In children: restitution of kidney function in > 90% of cases
- In adults, about 50% of patients suffer from persistently reduced renal function.