↓ Production of urine → ↑ extracellular fluid volume → total-body volume overload
↓ Excretion of waste products (e.g., urea, drugs)
↓ Excretion of phosphate → hyperphosphatemia
During the early stages of CKD, plasma phosphate levels will typically be normal due to the increased secretion of fibroblast growth factor 23 (FGF23).
FGF23 is produced by osteoblasts in response to initial hyperphosphatemia and increased calcitriol.
Increased secretion of FGF23 leads to increased phosphate secretion and suppressed conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D.
In advanced CKD, the effects of FGF 23 subside (most likely due to development of resistance in target tissues).
↓ Maintenance of acid-base balance → metabolic acidosis
↓ Hydroxylation of calcifediol → ↓ production of calcitriol → (in combination with ↓ excretion of phosphate) → ↓ serum Ca2+ → ↑ PTH
↓ Erythropoietin → ↓ stimulation of erythropoiesis
Clinical features
Manifestations of uremia
Definition: Uremia is defined as the accumulation of toxic substances due to decreased renal excretion. These toxic substances are mostly metabolites of proteins such as urea, creatinine, β2 microglobulin, and parathyroid hormone.
Uremic fetor: characteristic ammonia- or urine-like breath odor
Dermatological manifestations
Pruritus
Accumulation of histamine
Skin color changes (e.g., hyperpigmentation, pallor due to anemia)
Uremic frost: uremia leads to high levels of urea secreted in the sweat, the evaporation of which may result in tiny crystallized yellow-white urea deposits on the skin.
Serositis
Uremic pericarditis: a complication of chronic kidney disease that causes fibrinous pericarditis
Clinical features: chest pain worsened by inhalation
Physical examination findings
Friction rub on auscultation
ECG changes normally seen in nonuremic pericarditis (e.g., diffuse ST-segment elevation) are not usually seen.
Pleuritis
Neurological symptoms
Asterixis
Signs of uremic encephalopathy
Seizures
Somnolence
Coma
Peripheral neuropathy → paresthesias
Hematologic symptoms
Anemia
Leukocyte dysfunction → ↑ risk of infection
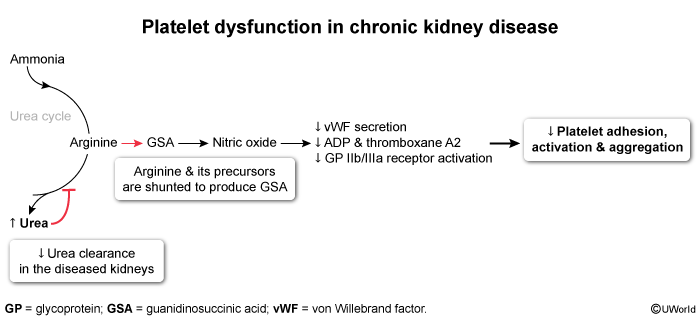
↑ Bleeding tendency caused by abnormal platelet adhesion and aggregation