Hashimoto disease is the most common form of thyroiditis and the most frequent cause of hypothyroidism in the US.
Iodine deficiency is the most common cause of hypothyroidism worldwide.
Sex: ♀ > ♂ (7:1)
Age of onset: occurs in all age groups; most prevalent in women aged 30–50 years
Etiology
Pathophysiology
Associations with HLA-DR3, and DR5 have been proposed.
Cellular (especially T cells) and humoral immune responses are activated → active B lymphocytes produce thyroid peroxidase antibodies (TPOAbs) and thyroglobulin antibodies (TgAbs) → destruction of thyroid tissue
Clinical features
Early-stage
Primarily asymptomatic
Goiter: nontender or painless, rubbery thyroid with moderate and symmetrical enlargement
Hashitoxicosis may occur: transient thyrotoxicosis due to follicular rupture of hormone-containing thyroid tissue that manifests with signs of hyperthyroidism (e.g., irritability, heat intolerance, diarrhea)
Late-stage
Thyroid may be normal-sized or small if extensive fibrosis has occurred.
Signs of hypothyroidism (e.g., cold intolerance, constipation, fatigue)
Diagnostics
Thyroid function tests (TFTs)
Early-stage: Transient hashitoxicosis may appear (↓ TSH, ↑ FT3, and ↑ FT4).
Progression: subclinical hypothyroidism (mildly ↑ TSH; normal FT3 and FT4)
Late-stage: overt hypothyroidism (↑ TSH; ↓ FT4 and ↓ FT3)
Thyroid antibodies
Anti-TPOAbs (formerly anti-microsomal antibodies): positive in up to 95% of patients
Anti-TgAbs: positive in 60–80% of patients
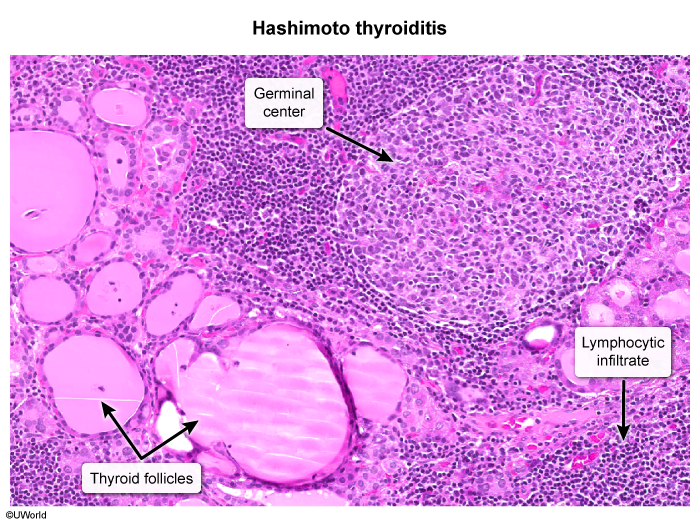
Fine-needle aspiration
Indications: patients with focal nodules to exclude malignancy (see “Workup of thyroid nodules”)
Findings: diffuse lymphocytic infiltration (cytotoxic T lymphocytes) with germinal centers, oncocytic-metaplastic cells (Hurthle cells), and fibrotic tissue t