Epidemiology
- Age of symptom onset: childhood
Etiology
Pathophysiology
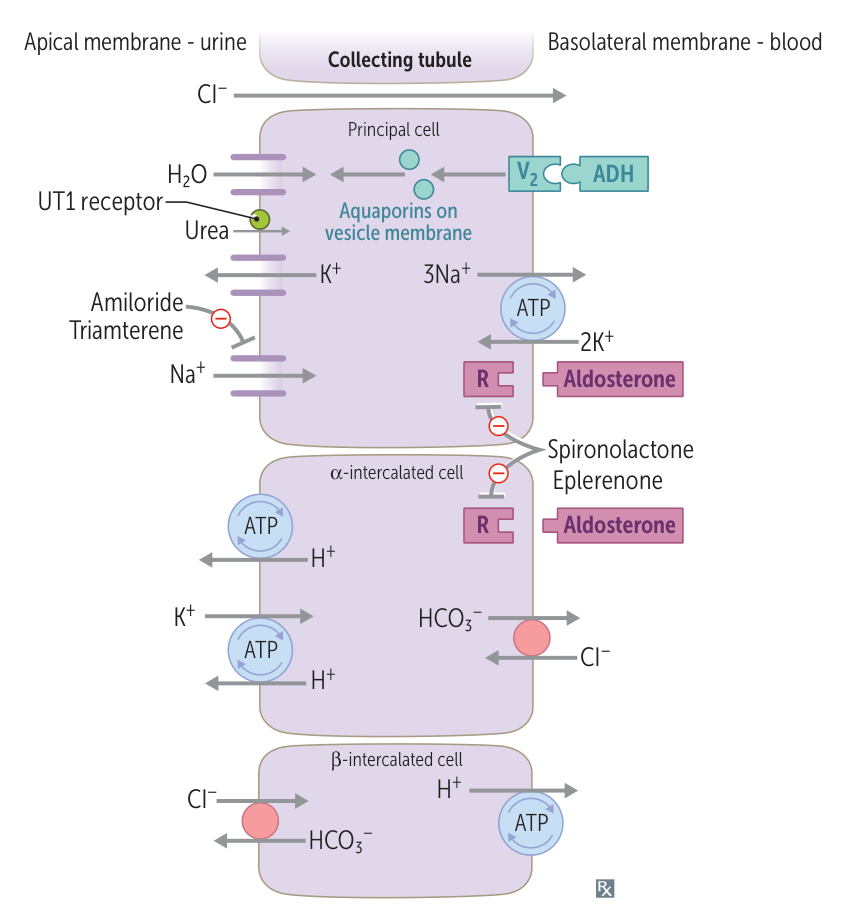
Structural alteration in the ENaC subunits → inability of these subunits to bind with an intracellular ubiquitin-protein ligase (Nedd4) → decreased degradation of ENaC channels by ubiquitin proteasomes → increased number of ENaCs in the collecting duct → increased reuptake of water and sodium (pseudohyperaldosteronism) → hypertension with low renin production and hypokalemia
ENaC
aka epithelial Na+ channel
Clinical features
Tip
The clinical features of Liddle syndrome are similar to those of hyperaldosteronism, except that Liddle syndrome manifests with decreased renin and aldosterone levels!
Diagnostics
- Hypokalemia
- Metabolic alkalosis
Treatment
Lifelong oral potassium substitution with potassium-sparing diuretics that directly block ENaCs in the collecting duct (e.g., amiloride, triamterene)
Warning
The potassium-sparing diuretic spironolactone (an aldosterone receptor antagonist) is not effective in Liddle syndrome because the increased sodium channel activity is not caused by aldosterone.