Epidemiology
Etiology
Pathophysiology
During fetal development, anterior and superior deviation of the infundibular septum → misaligned VSD with overriding aortic root and subsequent RVOTO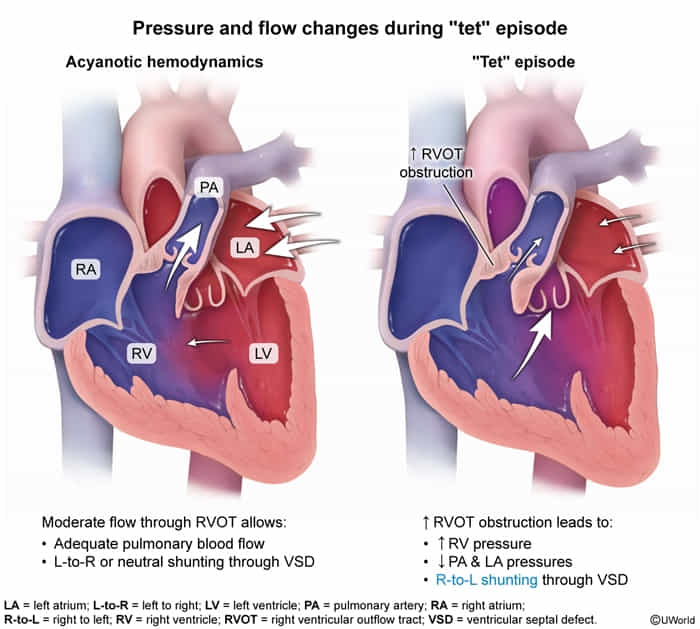
Clinical features
- Tet spells: intermittent hypercyanotic, hypoxic episodes with a peak incidence at 2–4 months after birth
- Associated with psychological and physical stress (e.g., crying, feeding, defecation)
- Caused by either an increase in pulmonary vascular resistance (PVR) or a decrease in systemic vascular resistance (SVR) → low SVR:PVR ratio allows the deoxygenated right ventricular output to take the low-resistance route to the systemic circulation, leading to acute hypoxemia (“Tet spell”).
- Spells occur suddenly and are potentially lethal.
- Untreated children tend to squat
- Squatting → ↑ SVR → ↓ right-to-left shunt → ↑ blood flow to pulmonary circulation → ↓ hypoxemia → relief of symptoms
- Cardiac examination findings
- Harsh crescendo-decrescendo systolic ejection murmur at the left upper sternal border
- Caused by pulmonary stenosis, not the associated VSD
- Single S2
- Possible RV heave and systolic thrill
- Harsh crescendo-decrescendo systolic ejection murmur at the left upper sternal border
Diagnostics
- Increased hematocrit: secondary polycythemia
Treatment
- Ductal-dependent CHDs: a group of CHDs that require the patent ductus arteriosus (PDA), which supplies either pulmonary or systemic circulation, to sustain life until surgery can be performed
- PDA supplies systemic circulation in the following:
- Transposition of the great arteries
- Hypoplastic left heart syndrome
- Coarctation of the aorta
- PDA supplies pulmonary circulation in the following:
- Tricuspid atresia
- Treatment: administration of prostaglandin E1 (PGE1) infusion
- Example: IV alprostadil infusion
- Mechanism of action: prevents the ductus arteriosus from closing, creating an intentional shunt to allow mixing of deoxygenated with oxygenated blood
- PDA supplies systemic circulation in the following: