Epidemiology
- Prevalence: second most prevalent skeletal disease after osteoporosis in individuals > 50 years of age
Etiology
Pathophysiology
Overview
Idiopathic disease
- Associated with a high rate of bone remodeling: ↑ RANKL-RANK activity → ↑ NF-κB signaling → ↑ osteoclast activity → ↑ osteoblast activity → formation of disorganized (woven) bone
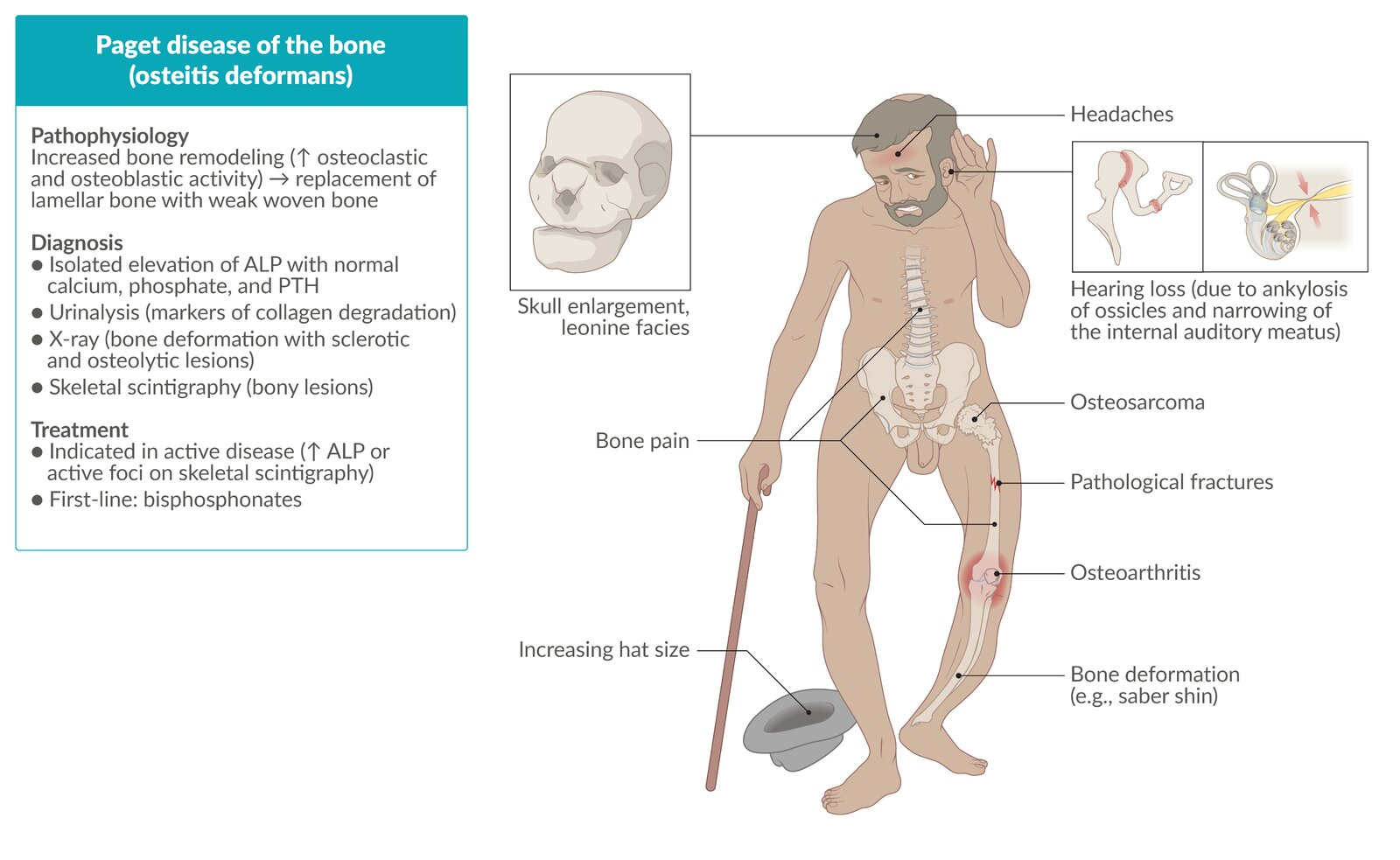
- The result is that newly remodeled bone is more vascular, and lacks the strength and shape of normal bone. This weak bone can be easily deformed by stress (e.g., weight bearing) and is highly susceptible to fractures. Furthermore, bone remodeling in Paget disease can result in enlargement of bone, which can result in entrapment neuropathies in regions where nerves pass through bony tunnels (e.g., cranial nerve canals, skull base foramina, spinal canal).
Stages of Paget disease
Bone remodeling in Paget disease occurs in three phases, followed by a quiescent stage:
- Lytic phase: ↑ number of osteoclasts appear in bone → ↑ osteoclastic activity → ↑ rate of bone resorption
- Mixed lytic and blastic phase: ↑ osteoclastic activity is accompanied by an ↑ number of osteoblasts, which infiltrate the lacunae → ↑ rate of bone formation with haphazardly laid collagen fibers → formation of abnormal hypervascular woven bone
- Sclerotic phase: Osteoblastic activity overtakes osteoclastic activity, which leads to formation of dense, sclerotic bone.
- Quiescent stage: Both osteoclastic and osteoblastic activity cease (“quiet phase” of the disease).
Disease localization
The pelvis, skull, vertebral column, and long bones of the lower extremities are the most commonly affected sites.
Clinical features
- Approximately 70–90% of cases are asymptomatic.
- Bone pain, which may be associated with erythema and elevated skin temperature over the affected bones
- Due to increased vascularity of the underlying bone.
- Pathological fractures: chalk-stick fractures of long bones
- Bony deformities, e.g., bowing of legs (saber shin)
- Skull involvement (in ∼ 40% of cases)
- Skull enlargement (increasing hat size)
- Cranial nerve deficits
- Impaired hearing: due to ankylosis of the ossicles and narrowing of the internal auditory meatus
- Vertebral involvement: Cauda equina syndrome, nerve root compression, spinal stenosis
Diagnostics
- Radiographs typically reveal lytic or mixed lytic-sclerotic lesions, thickening of cortical and trabecular bone, and bony deformities.
- Serum total ALP: often significantly increased; first-line test to assess disease severity
- Due to increased osteoblast activity
- Serum calcium, phosphate, and parathyroid hormone (PTH) levels: typically normal
- Normal homeostasis is usually maintained despite the bone remodeling involved in PDB.
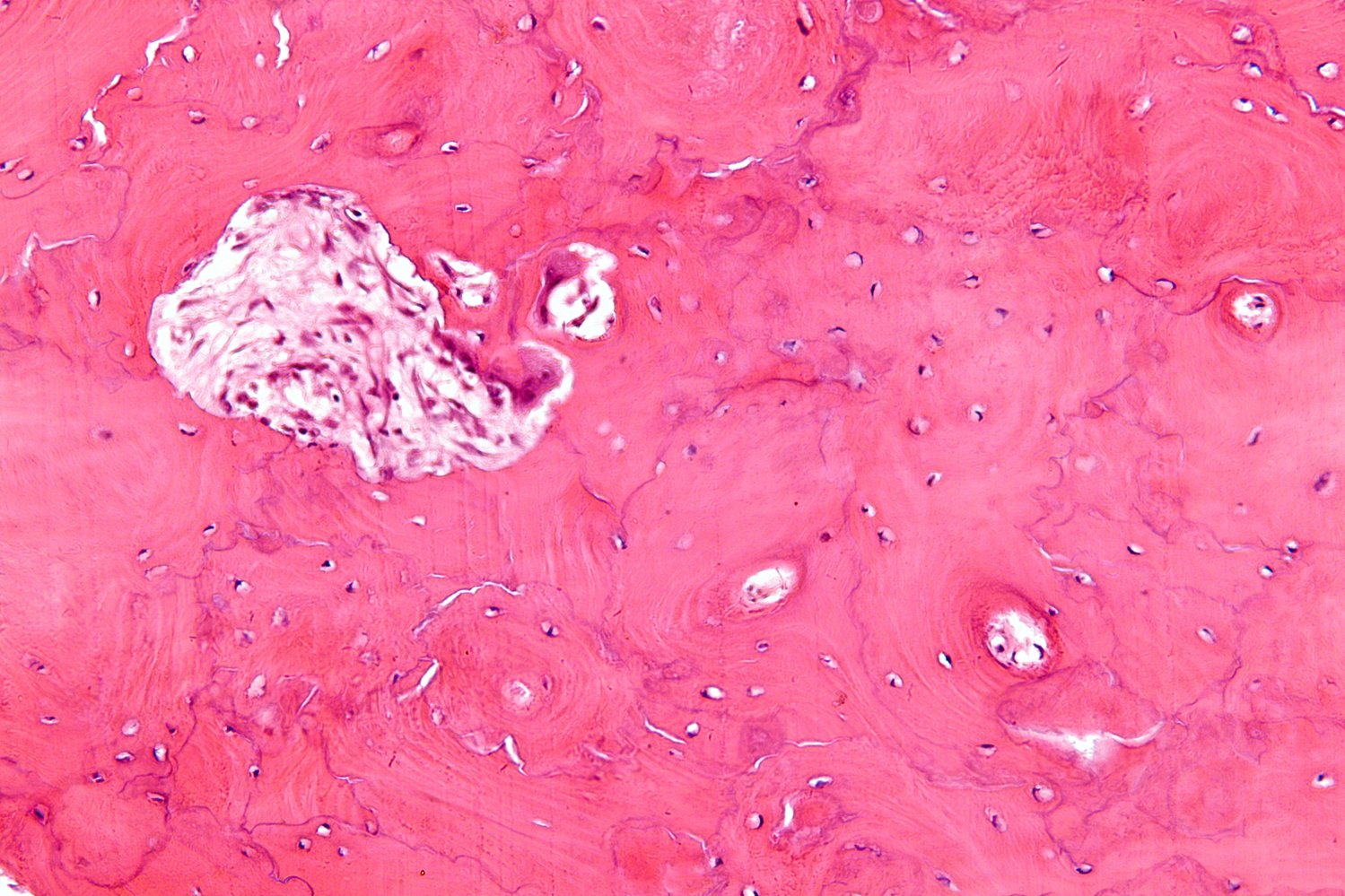
- Bone biopsy
- Typically shows a chaotic, mosaic-like pattern of irregularly juxtaposed lamellar and woven bone
- Typically shows a chaotic, mosaic-like pattern of irregularly juxtaposed lamellar and woven bone
Treatment
Bisphosphonates
- First-line therapy for patients with bone pain and those at risk of bone complications
- Mechanism: induce apoptosis of osteoclasts
- Bisphosphonates are pyrophosphate analogs that bind to hydroxyapatite binding sites on the surface of bone tissue: uptake by osteoclasts during phases of bone resorption → interference with osteoclast function and promotion of osteoclast apoptosis → reduced bone resorption
- Used to treat hypercalcemia and bone metabolism disorders (e.g., osteoporosis or tumor-induced osteolysis).
- Examples include zoledronic acid, pamidronate, etidronate, and alendronate.
- Adverse effects
- Bisphosphonate-related osteonecrosis of the jaw: adverse effect of bisphosphonates, usually seen with high-dose IV administration in tumor patients
- Etiology: Trauma to the jaw (e.g., tooth extractions or other dental procedures) is a trigger in many cases.
- Pathophysiology: not yet fully understood
- Clinical features: chronic swelling, mild pain, exposed necrotic bone
- Treatment: supportive, e.g.,:
- Improving oral hygiene
- Antibiotic rinses
- Limited debridement
- Prevention
- Dental examination in conjunction with treatment of preexisting dental conditions (e.g., extraction of unrestorable teeth) prior to initiation of therapy
- Establishing a daily oral care plan that involves daily oral rinsing, brushing, and flossing
- Esophageal inflammation and cancer
- To avoid this complication, patients should swallow medication with a sufficient amount of water and maintain an upright position for 30 minutes.
- Bisphosphonate-related osteonecrosis of the jaw: adverse effect of bisphosphonates, usually seen with high-dose IV administration in tumor patients