- Disruption of the ipsilateral sympathetic chain supplying the head, eye, and neck.
- Results from a lesion anywhere along the three-neuron sympathetic pathway.
Pathophysiology
Central
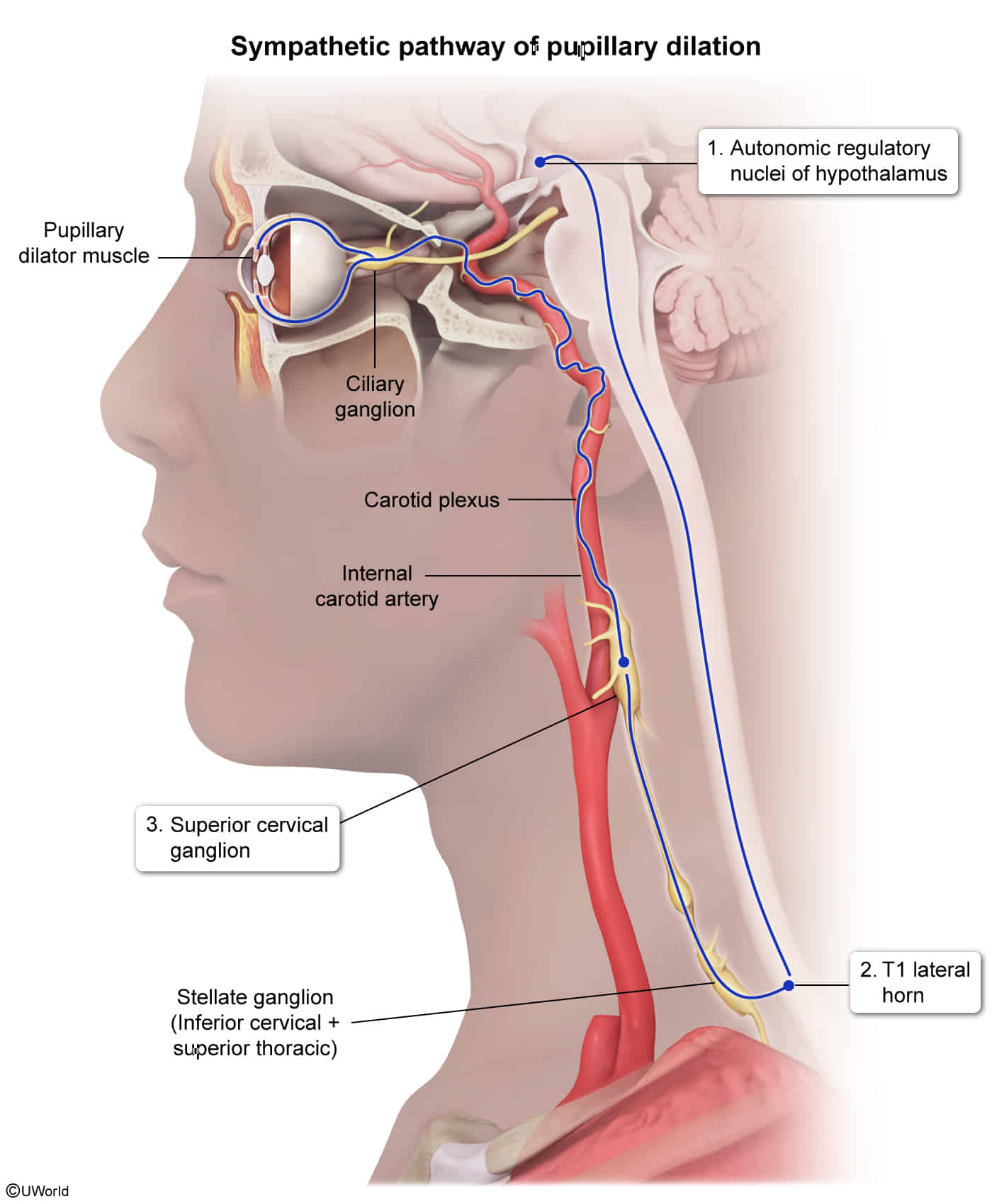
- Anatomical trajectory: Hypothalamus (first-order oculosympathetic neuron) → brainstem, cervical, and thoracic spinal cord → ciliospinal center (C8–T2)
- Typical lesions:
Preganglionic
- Anatomical trajectory: Ciliospinal center (second-order oculosympathetic neuron) → pulmonary apex → stellate ganglion → superior cervical ganglion
- Typical lesions:
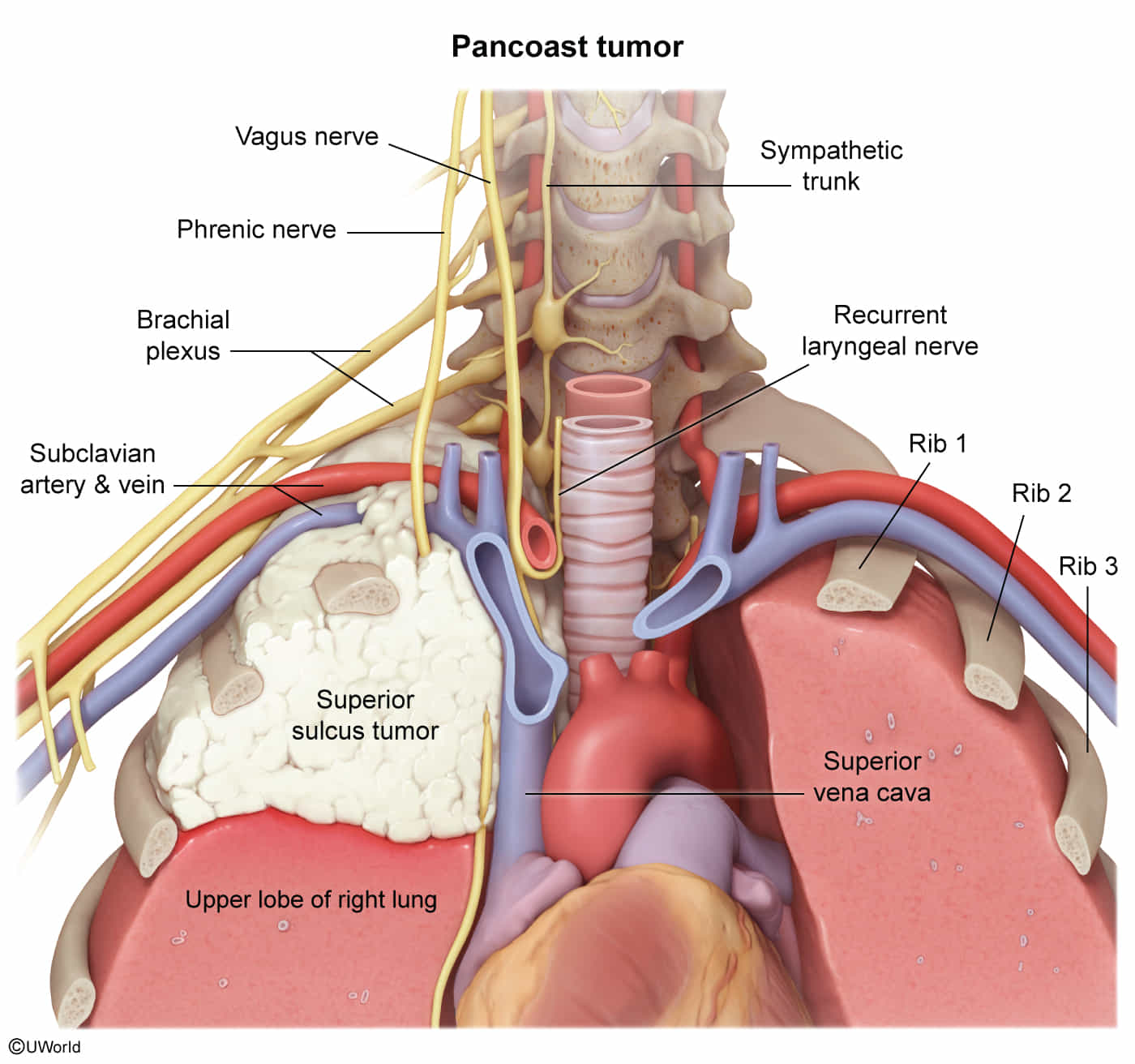
- Tumors (e.g., breast or lung cancer compressing stellate ganglion, esp. Pancoast tumor)
- Iatrogenic (e.g., birth trauma, central venous catheterization)
- Lymphadenopathy
- Arterial lesions/dissection: aorta, subclavian, common carotid
- Cervical rib
Postganglionic
- Anatomical trajectory: Superior cervical ganglion (third-order oculosympathetic neuron) → internal carotid artery and ophthalmic nerve → iris dilator muscle
- Typical lesions:
Clinical features
- Triad of Horner syndrome
- Miosis (constriction of the pupil)
- Occurs because the sympathetically controlled iris dilator muscle fails to contract. See Pupillary light reflex.
- Leads to anisocoria and a dilation lag on exam
- More noticeable in the dark when the sympathetic tone is increased
- Partial ptosis (drooping of the upper eyelid)
- Occurs because the sympathetically controlled superior tarsal muscle fails to keep the upper eyelid raised
- It is milder than ptosis associated with oculomotor nerve or levator palpebrae muscle lesions.
- Anhidrosis (absence of sweating) or reduced sweating on the face and arm, depending on the location of the lesion
- Occurs because the sympathetic innervation of the facial Hair follicles and glands is impaired
- Seen in central and preganglionic lesions
- Facial flushing due to vasodilatation
- Occurs because the vasoconstrictive effect of the sympathetic nervous system is lost.
- (Apparent) enophthalmos
- Associated symptoms depending on the etiology:
- Atrophy of arm and hand muscles
- Infiltration of the brachial plexus causes pain (plexus neuralgia), as well as motor and sensory deficits in the arm.
- Pain in the neck or face