↑ ICP → ↓ CPP → compensatory activation of the sympathetic nervous system → ↑ systolic blood pressure → stimulation of aortic arch baroreceptors → activation of the parasympathetic nervous system (vagus) → bradycardia
↑ Pressure on brainstem → dysfunction of respiratory center → irregular breathing
Clinical features
Global
Cushing triad: irregular breathing, widening pulse pressure, and bradycardia
Increase in systolic, decrease in diastolic blood pressure
Reduced levels of consciousness
Headache
Vomiting
Papilledema
Psychiatric changes
In infants: macrocephaly, bulging fontanel, sunset sign
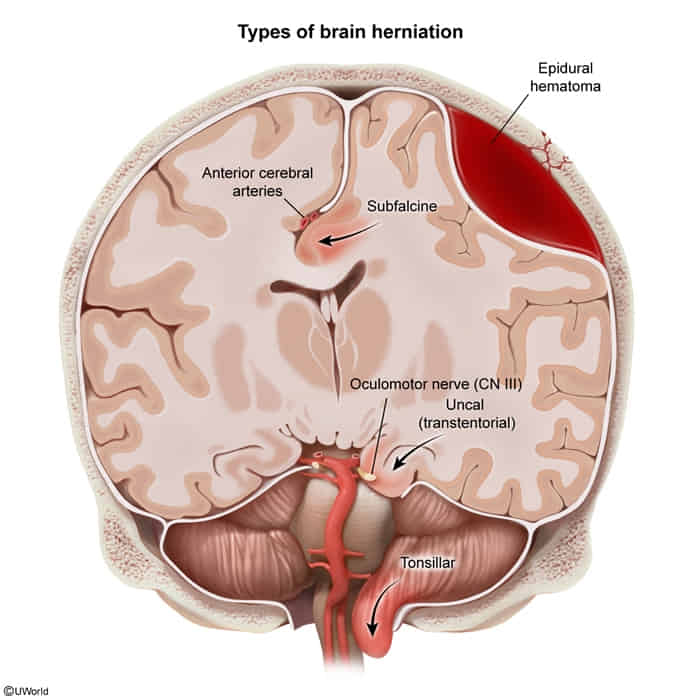
Subtypes
Subfalcine
Herniation of cingulate gyrus underneath falx cerebri
No pupillary involvement, consciousness often preserved
Contralateral leg weakness (ipsilateral ACA compression)
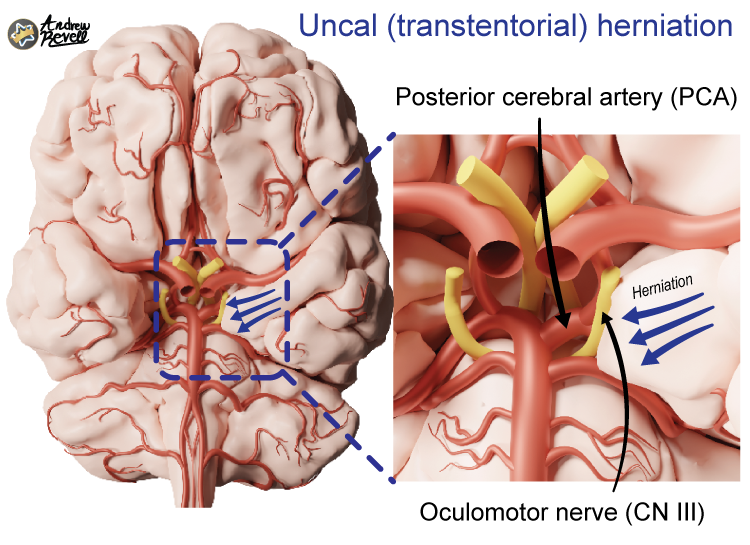
Uncal
Herniation of uncus (medial temporal lobe) under tentorium cerebelli