Epidemiology
Etiology
- Dihydrotestosterone (DHT) is a potent prostatic growth factor.
- Androgen-estrogen imbalance: As men age, testosterone levels decline, but estrogen levels remain the same, which results in a higher estrogen/testosterone ratio.
Pathophysiology
Clinical features
Diagnostics
Serum PSA level
- Findings
- Total PSA > 1.5 ng/mL: suggests an enlarged prostate (> 40 mL)
- Total PSA > 4 ng/mL: increased likelihood of prostate cancer
- Free PSA levels and free PSA/total PSA ratio
- ↑ Free PSA levels and ↑ free PSA/total PSA ratio: usually seen in BPH
- ↓ Free PSA levels and ↓ free PSA/total PSA ratio: suggestive of prostate cancer
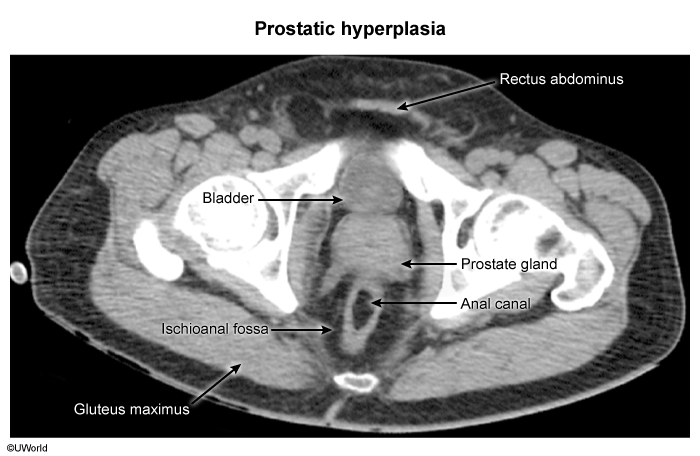
MRI and CT pelvis
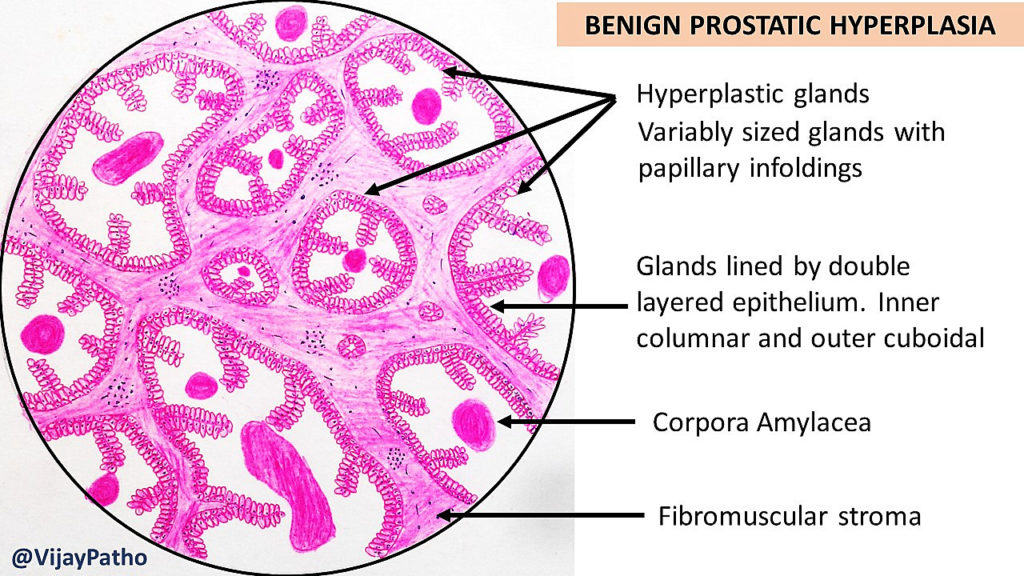
Pathology
- Nodular hyperplasia of glandular and stromal elements. t
- Microscopic: Corpora amylacea (calcified proteinaceous concretions) may be seen (nonspecific).
Treatment
Pharmacological therapy
Uroselective alpha-1 blockers
- Tamsulosin, Doxazosin, Alfuzosin, Terazosin
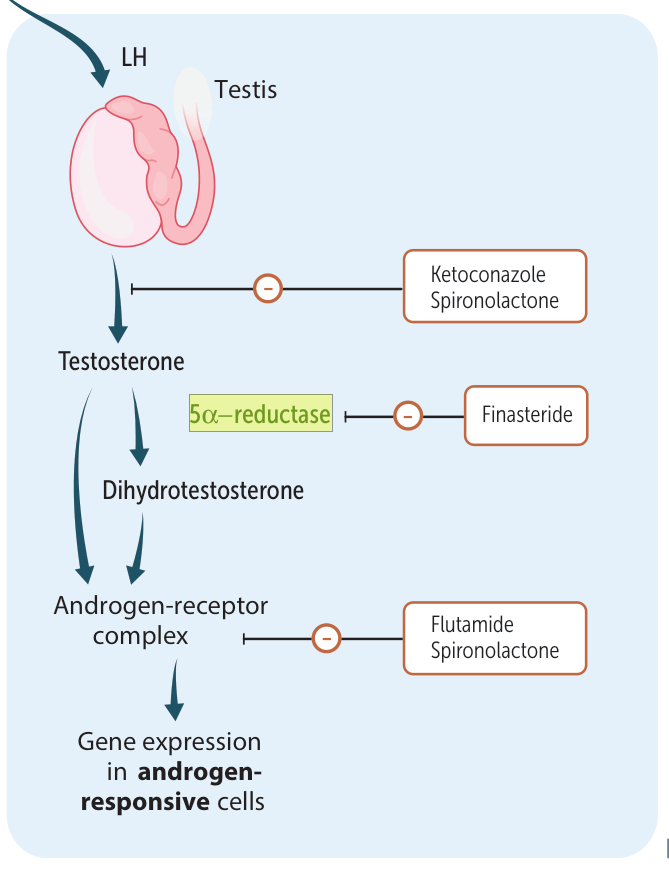
5-alpha reductase inhibitors (5-ARIs)
Important
Only DHT has a promoting effect on the prostate, testosterone does not. Therefore we use 5-alpha reductase inhibitors to inhibit the conversion of testosterone to DHT.
- See Adrenal androgen synthesis
- Inhibition of 5-alpha reductase → ↓ conversion of testosterone to DHT → ↓ intraprostatic DHT levels → ↓ prostatic growth and ↑ prostatic apoptosis and involution → improvement of LUTS
- Adverse effects: sexual dysfunction (e.g., erectile dysfunction, decreased libido, ejaculatory dysfunction), gynecomastia
- Finasteride, Dutasteride
Tip
-steride (“testosterone reductase inhibitor”)
Phosphodiesterase type 5 inhibitors (PDE-5 inhibitors)
- Increase in intracellular cGMP → ↓ detrusor, prostate, and urethra muscle tone → improvement of LUTS
- Tadalafil
Complications
- Recurrent UTI
- BPH → incomplete voiding → urinary stasis → predisposition to UTIs
- Urinary retention with bladder distension and bladder wall thickening (hypertrophy)
- Bladder calculi
- Hydronephrosis
- Chronic kidney disease