Nonsteroidal anti-inflammatory drugs (NSAIDs)
Agents
- Ibuprofen
- Diclofenac
- Indomethacin
- Naproxen
- Piroxicam
- Meloxicam
- Ketorolac
- Sulindac
- Aspirin
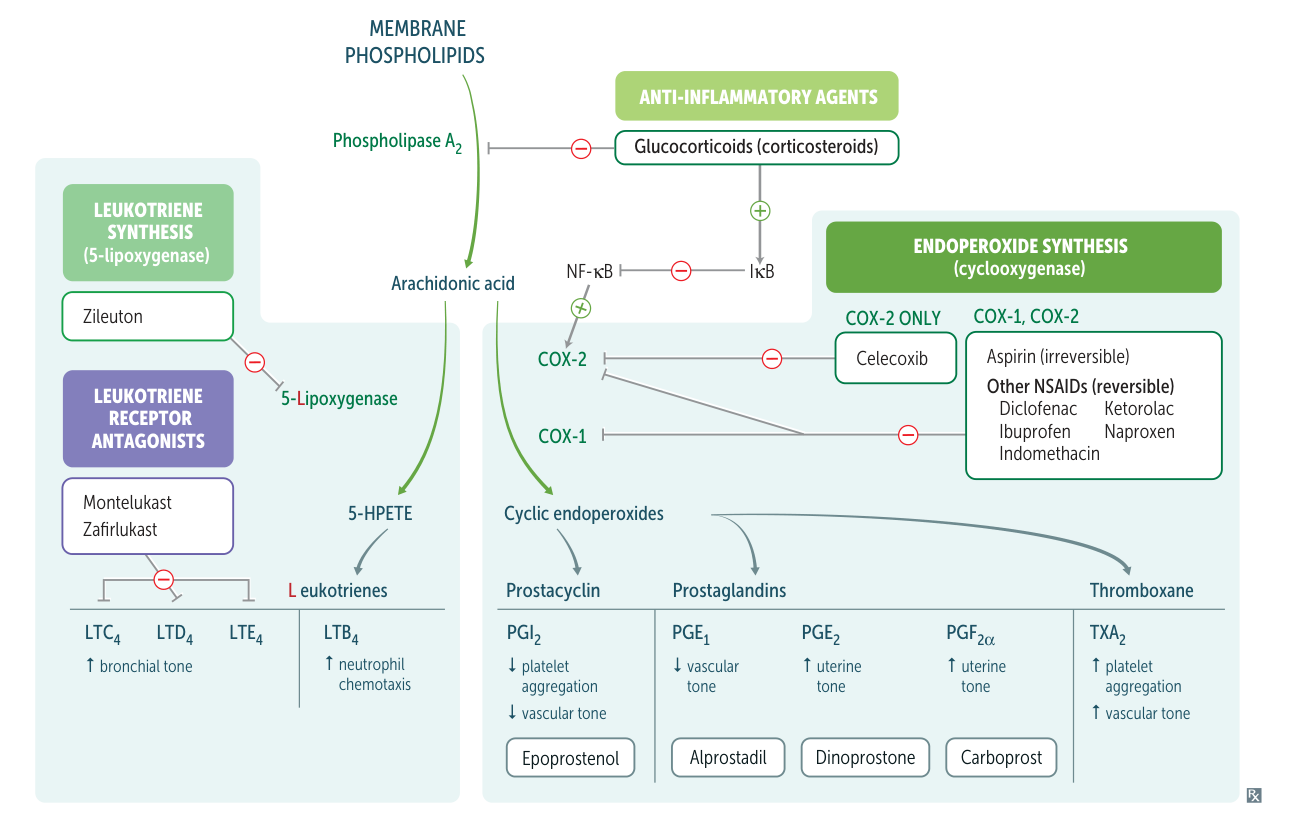
Mechanism of action
- Reversible inhibition of the enzymes COX-1 and COX-2 → decreased prostaglandin synthesis
- Aspirin is the exception, because it leads to irreversible COX-1 and COX-2 inhibition.
Choice
- Acetaminophen
- For mild to moderate pain
- Safe
- Can be used by children and pregnant women
- Ibuprofen
- For acute, mild to moderate pain
- Works fast
- Naproxen
- Strong and long-lasting
- May affect wound healing
- Aspirin
- Only salicylate among NSAIDs
- Commonly used as antiplatelet agents, instead of Pain management or anti-inflammatory agents
- See Salicylate poisoning for overdose effects
- For mild to moderate pain accompanied by swelling and inflammation, non-steroidal anti-inflammatory drugs (such as ibuprofen, aspirin, and naproxen) are more effective.
Selective COX-2 inhibitors
Agent
Celecoxib
Mechanism of action
Reversible selective inhibition of COX-2 with almost no inhibition of COX-1
Mnemonic
Selecoxib
Effects
- Analgesic and anti-inflammatory
- Advantages in comparison to nonselective NSAIDs
- No antiplatelet effect: platelets only possess COX-1 and are therefore not targeted by selective COX-2 inhibitors. This means that the activity of thromboxane A2 (TXA2) is not interrupted (TXA2 normally promotes platelet aggregation).
- Gastric mucosal cells express mostly COX-1, which is involved in maintaining a healthy gastric mucosa, so there are minimal gastrointestinal side effects and a lower risk of gastric ulcers.
Indications
Other non-opioid Pain management
Agent
Acetaminophen
Mechanism of action
- Reversibly inhibits cyclooxygenase, mainly in the CNS
- Inactivated peripherally
Effects
- Antipyretic
- Analgesic
- No anti-inflammatory effect
Side effects
- Hepatotoxicity due to acetaminophen overdose (drug-induced hepatitis)
- Leading cause of acute hepatic failure in the US
- Pathophysiology
- Exhaustion of hepatic metabolic pathways causes increased formation of a toxic metabolite of acetaminophen, N-acetyl-p-benzoquinoneimine (NAPQI).
- Glutathione initially inactivates NAPQI, but its reserves are eventually depleted, leading to NAPQI build-up.
- NAPQI → irreversible oxidative hepatocyte injury → liver cell necrosis
- Exhaustion of hepatic metabolic pathways causes increased formation of a toxic metabolite of acetaminophen, N-acetyl-p-benzoquinoneimine (NAPQI).
- Clinical features
- Nonspecific symptoms (nausea, vomiting, pallor lethargy) or asymptomatic in the first 24 hours after ingestion
- Progressive liver impairment (RUQ pain, liver enlargement and tenderness, abnormal liver function tests)
- If acute liver failure does not develop, patients typically begin to recover within 2 weeks after ingestion.
- Acute kidney failure occurs in approx. 50% of patients with acute hepatic failure.
- Antidote: PO or IV N-acetylcysteine (NAC)
- NAC replenishes glutathione stores in the liver