- Epidemiology
- Most common in individuals 50–70 years of age
- Etiology
- Genetic susceptibility
- Presence of a genetic mutation that causes decreased acetyltransferase activity, which results in the slow acetylation of drugs
- Drug triggers
- High risk: procainamide and hydralazine
- Low risk: sulfa drugs and certain nonsulfa drugs, (e.g., isoniazid, methyldopa, minocycline, phenytoin, TNF-α inhibitors)
- Genetic susceptibility
- Clinical features (usually manifest ≥ 1 month after medication initiation)
- Constitutional: fatigue, fever, and weight loss
- Musculoskeletal: myalgia and symmetrical polyarthralgia
- Skin lesions (e.g., malar rash)
- Diagnostics
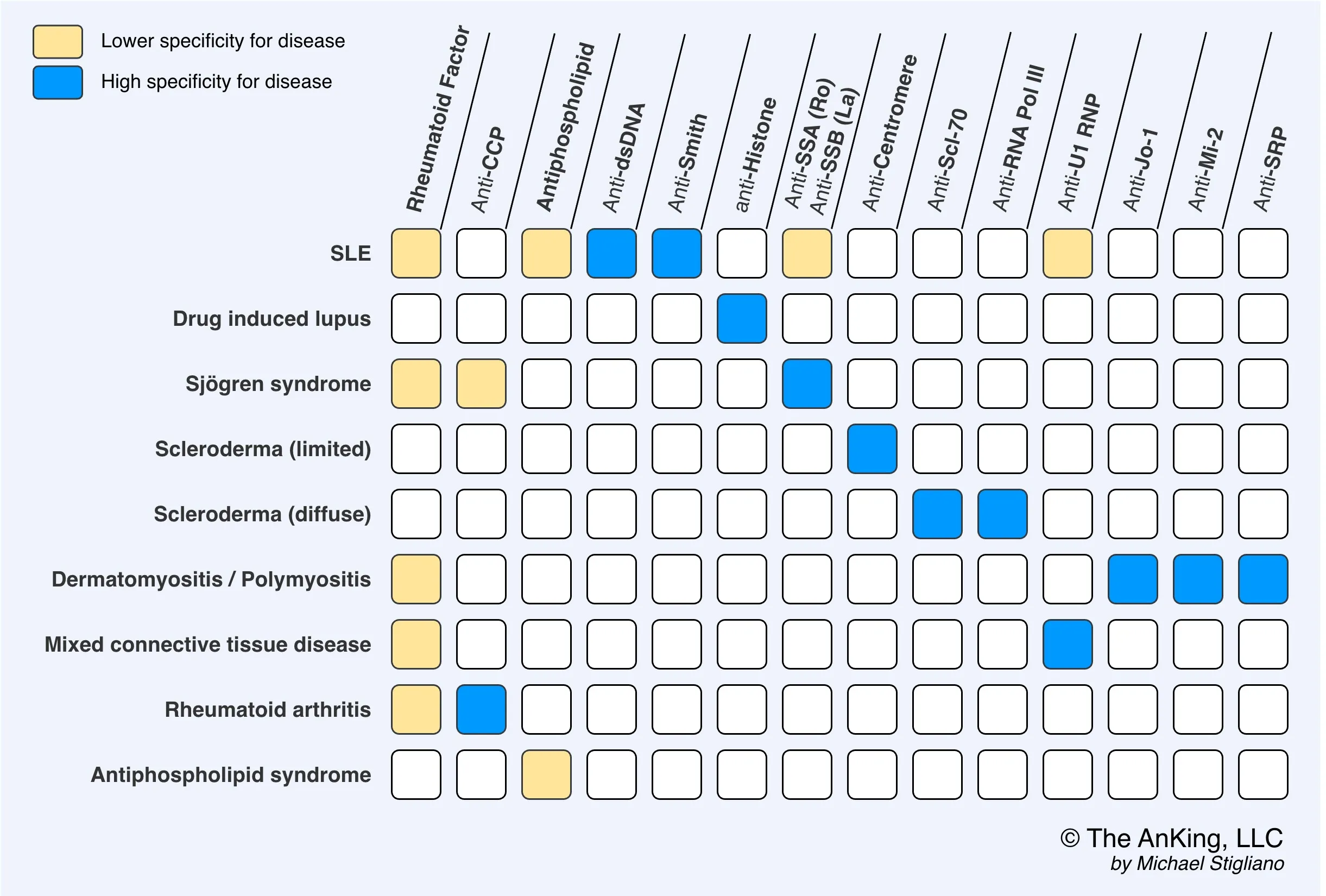
- ANAs are positive in nearly all patients.
- Antihistone antibodies
- Antihistone antibodies are seen in 90–95% of patients.
- Antihistone antibodies are seen in 90–95% of patients.
Tip
DILE can manifest with various features that are also seen in idiopathic SLE (e.g., fever, arthritis, malar rash, serositis) but typically does not affect the CNS or kidneys, unlike SLE.