↑ Androgens during puberty → increased production of sebum by sebaceous glands
In women: menstrual cycle
Acne usually worsens the week before menstruation begins. The increase of progesterone can make the skin secrete more oil.
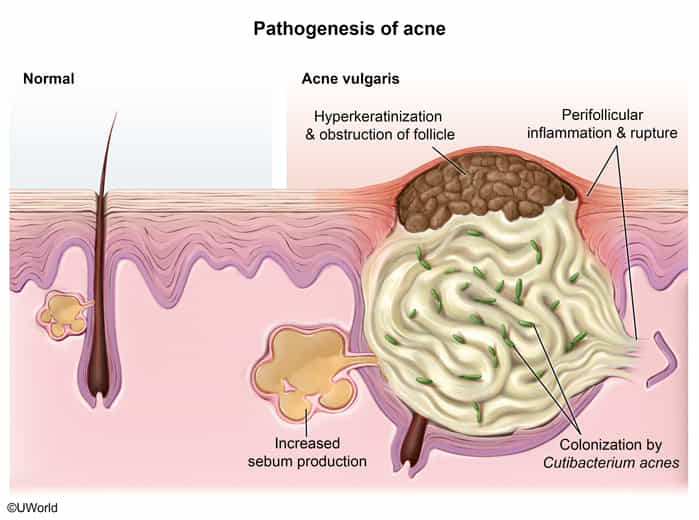
Follicular hyperkeratosis: Higher keratinocyte activity and decreased keratinocyte shedding in pilosebaceous units leads to the formation of comedones.
Bacterial colonization with Cutibacterium acnes (formerly known as Propionibacterium acnes) → inflammatory reactions with formation of papules, nodules, pustules, and/or cysts
Hyperkeratinization due to abnormal epithelial growth and differentiation of corneocytes leads to keratin plug formation in the pilosebaceous follicles. These blocked follicles are referred to as comedones (ie, whiteheads and blackheads).
In response to androgen stimulation (eg, during pubertal adrenarche), sebaceous glands enlarge (not involute) and increase production of sebum, a lipid-rich substance that facilitates obstruction of pilosebaceous follicles (Choice A).
Cutibacterium acnes, an anaerobic bacteria that relies on sebum as a nutrient source, proliferates in occluded follicles, triggering an inflammatory response that results in the red papules and pustules characteristic of nodulocystic acne.
Clinical features
Commonly found in areas with sebaceous glands (predilection sites: face, shoulders, upper chest, and back)
Noninflammatory acne: comedonal acne
Open comedones (“blackheads”): dark, open portion of sebaceous material
Closed comedones (“whiteheads”): closed small round lesions that contain whitish material (sebum and shed keratin)
Inflammatory acne: Affected areas are red and can be painful.
Papular/pustular acne: papules, pustules that arise from comedones
Nodulocystic acne (> 5 mm in diameter)
Commonly affects the back and neck
Diagnostics
Treatment
Mild acne
Topical treatment with any of the following:
Benzoyl peroxide
Retinoid
Moderate acne
Combination topical therapy for acne
OR a combination of:
Oral antibiotic for acne
AND topical:
Retinoid
Benzoyl peroxide
PLUS antibiotic if needed
Severe acne
Oral isotretinoin (preferred)
Topical retinoids
Retinoids are vitamin A derivatives with an anti-inflammatory and comedolytic effect.
Increase epithelial mitosis and desquamation, and help extrude debris from comedones, limiting acne formation.
Used as monotherapy for comedonal acne or adjunctive therapy for acne of any severity