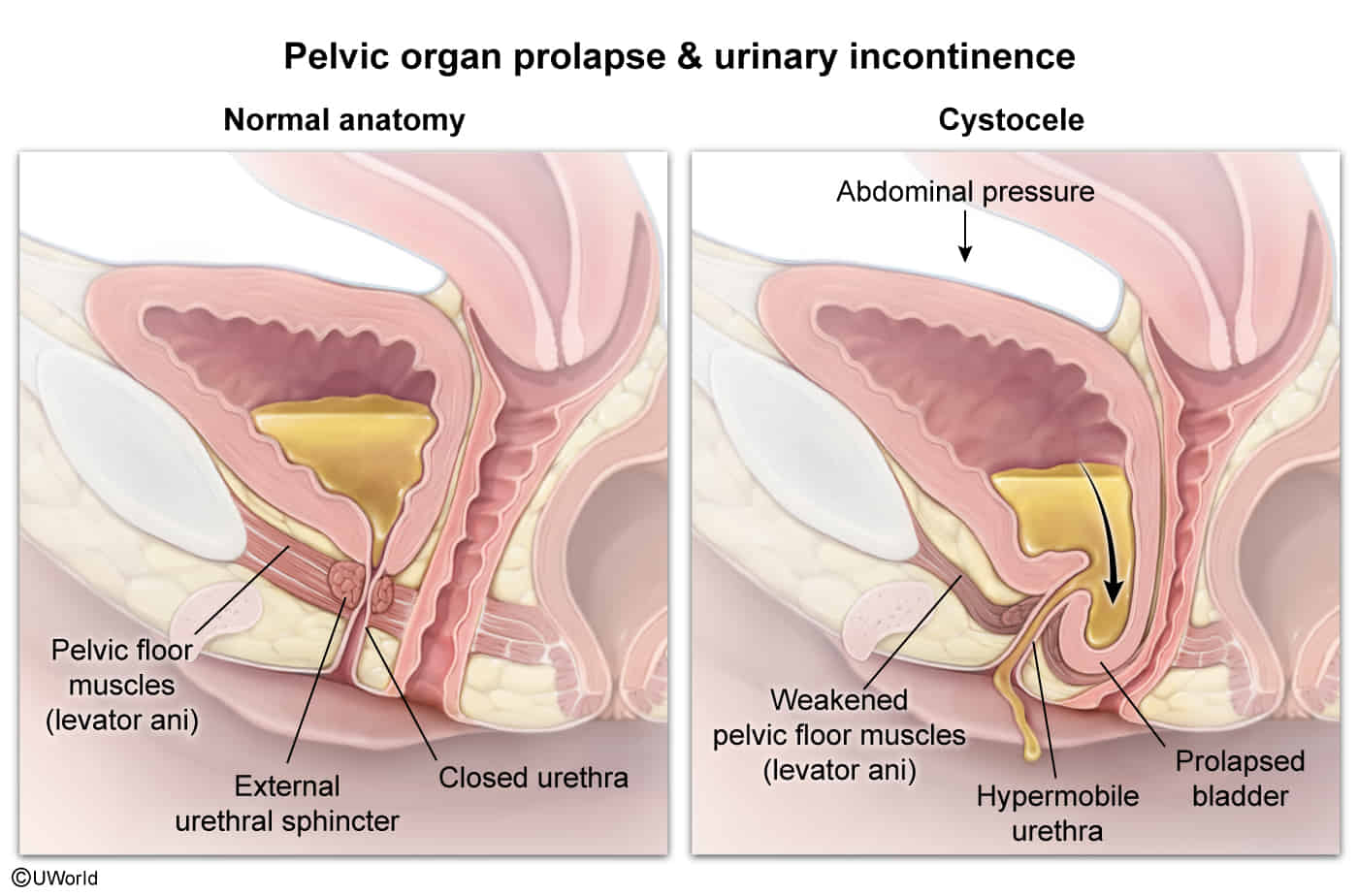
Increased intraabdominal pressure (due to, e.g., obesity, cough related to chronic lung disease and/or smoking, ascites, pelvic tumors, constipation)
Pathophysiology
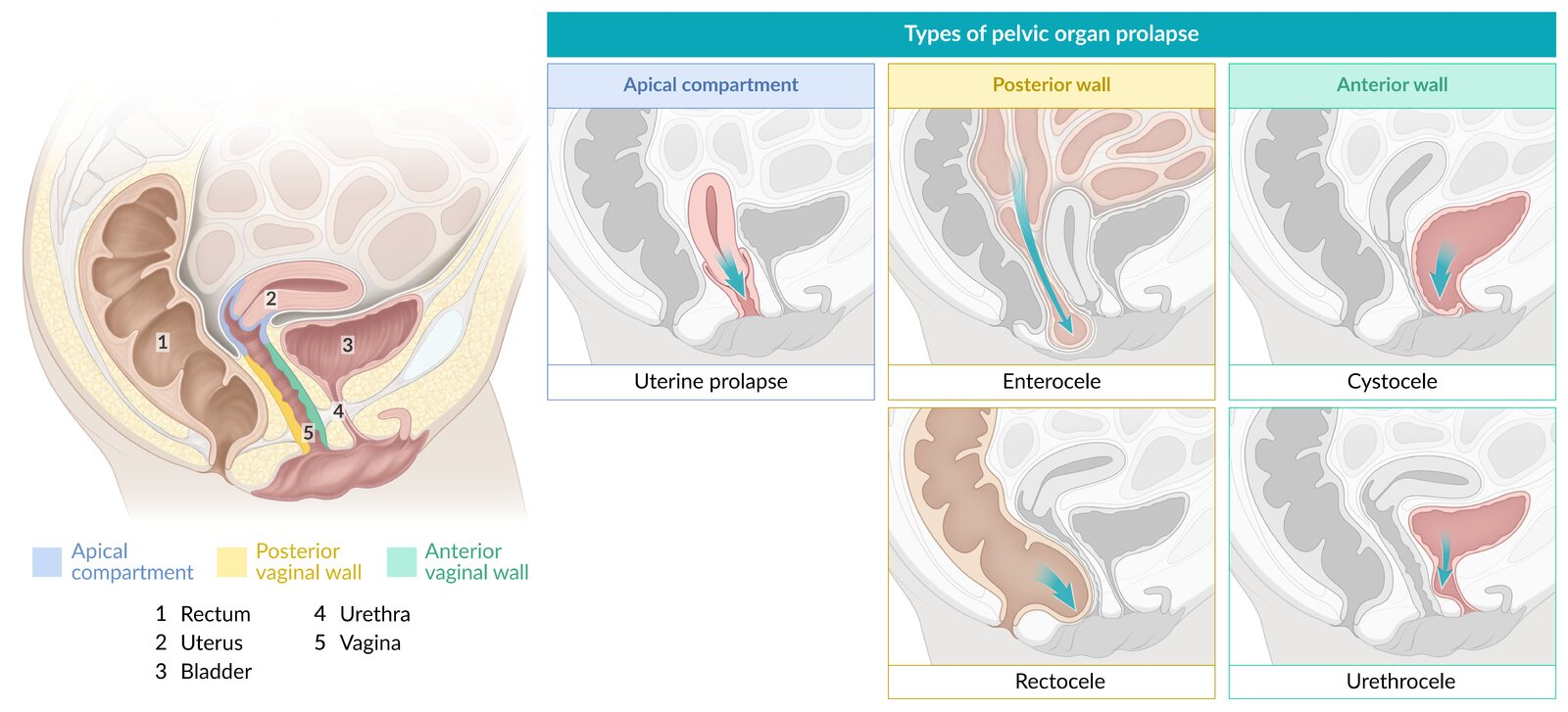
Specific sites
Vaginal wall prolapse
Anterior vaginal wall prolapse: herniated anterior vaginal wall, which is often associated with a cystocele (descent of the bladder) or urethrocele (descent of the urethra); can be due to weakness of the pubocervical fascia; Most common type.
Posterior vaginal wall prolapse: herniated posterior vaginal wall, which is associated with a rectocele (descent of the rectum) or enterocele (herniated section of the intestines); can be due to weakness of the rectovaginal fascia
Uterine prolapse: descent of the uterus
Vaginal vault prolapse: descent of the apex of the vagina
Apical compartment prolapse: herniated uterus, cervix, or vaginal vault
Uterine procidentia: protrusion of all vaginal walls or cervix beyond the vaginal introitus
Clinical features
Feeling of pressure on or discomfort around the perineum (“sensation of vaginal fullness”)
Lower back and pelvic pain (may become worse with prolonged standing or walking)