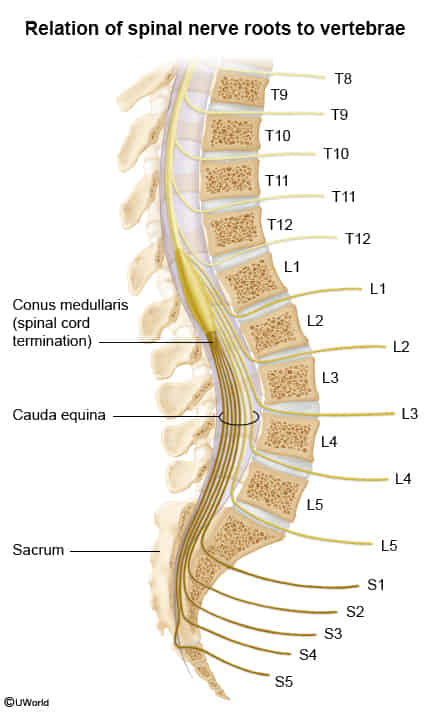
In an adult, the spinal cord terminates in a tapering fashion as the conus medullaris (T12-S4) at the L1-L2 vertebral level. The collection of spinal nerves below this point (eg, L3-S4) exit inferiorly through their respective intervertebral foramina and are referred to as the cauda equina (ie, horse’s tail).
It constitutes a surgical emergency as delayed treatment can lead to irreversible neurological damage, including paralysis and incontinence.
Most common cause: Massive central lumbar disc herniation, typically at L4/L5 or L5/S1.
Other causes: Spinal stenosis, tumors (metastatic or primary), trauma/fractures, spinal epidural abscess, or epidural hematoma.
Functions
Innervates the lower limb, perineum, and pelvic organs
Innervates the internal and external anal sphincter
Provides parasympathetic innervation to the bladder
Clinical features
Saddle Anesthesia: Sensory loss in the perineal region (S3-S5 distribution).
Bowel/Bladder Dysfunction:
Urinary retention (most sensitive sign; usually leads to overflow incontinence).
Hyporeflexia or areflexia (e.g., loss of ankle jerk).
Sexual dysfunction (erectile dysfunction).
Diagnosis
Clinical Suspicion: Diagnosis is suspected based on the characteristic history and physical exam findings. There should be a low threshold for investigation.
Imaging:Urgent MRI is the gold standard and is required to confirm the diagnosis and identify the cause of compression.
CT Myelogram can be used if MRI is contraindicated or unavailable.
Management
Surgical Emergency: Immediate hospital admission and neurosurgical consultation are required.
Treatment:Urgent surgical decompression (e.g., laminectomy) is the definitive treatment to relieve pressure on the nerve roots.
Timing: Surgery is ideally performed as soon as possible, with better outcomes generally seen if done within 24-48 hours of symptom onset.
Adjunctive Tx: High-dose corticosteroids may be used to reduce inflammation and swelling.
Key Associations/Complications
Prognosis: Even with prompt surgery, recovery is variable. Permanent deficits can include urinary/bowel incontinence, sexual dysfunction, chronic pain, and leg weakness.
CES-I vs. CES-R:
CES-I (Incomplete): Patient has altered urinary sensation but no established urinary retention. This has a better prognosis if operated on urgently.
CES-R (Retention): Patient has painless urinary retention and overflow incontinence. Prognosis is significantly worse.