Pathophysiology
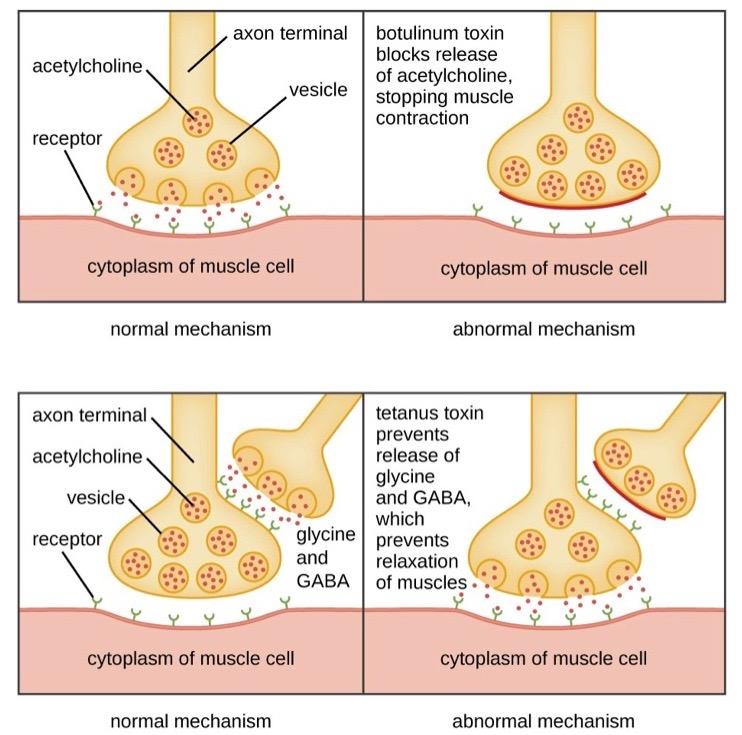
Botulinum toxin: protease that cleaves SNARE proteins and prevents fusion of transmitter-containing vesicles with the presynaptic membrane → inhibition of acetylcholine release from the presynaptic axon terminals
Tetanus vs botulism
Both work on SNARE proteins
Clinical features
- Neurological symptoms
- Descending paralysis
- Peripheral flaccid muscle paralysis that descends caudally (typically begins in frequently used muscles)
- Pupils: accommodation paralysis, mydriasis, diplopia
- Pharynx: dysarthria, dysphagia
- Infantile hypotonia (see “Infant botulism” below)
- Descending paralysis
- Gastrointestinal symptoms
- Gastrointestinal discomfort, nausea, and vomiting, later followed by constipation
Foodborne botulism
- Etiology
- Ingestion of preformed botulinum toxin via contaminated foods
- The anaerobic spores survive in poorly pasteurized canned foods (e.g., vegetables with soil contact, meat, home-fermented tofu)
- Germination of the spores produces dangerous toxins (botulinum toxins = enterotoxins A-F) and gas → bulging cans
- Ingestion of preformed botulinum toxin via contaminated foods
Infant botulism
- Etiology: ingestion of spores
- Spores may be present in honey, juice, and contaminated soil.
- Germination of the spores in intestinal tract → synthesis of botulinum toxin
- A mature immune system destroys spores before they can colonize the intestinal tract. Because the immune system is underdeveloped in the first year of life, the bacteria are able to colonize and produce the toxin inside an infant’s intestinal tract following ingestion.
- Incubation period: days to 4 weeks
- Clinical features: Infants may present with infantile hypotonia
- Age <12 months
- Constipation, poor feeding, hypotonia
- Oculobulbar palsies (eg, absent gag reflex, ptosis)
- Symmetric, descending paralysis