Epidemiology
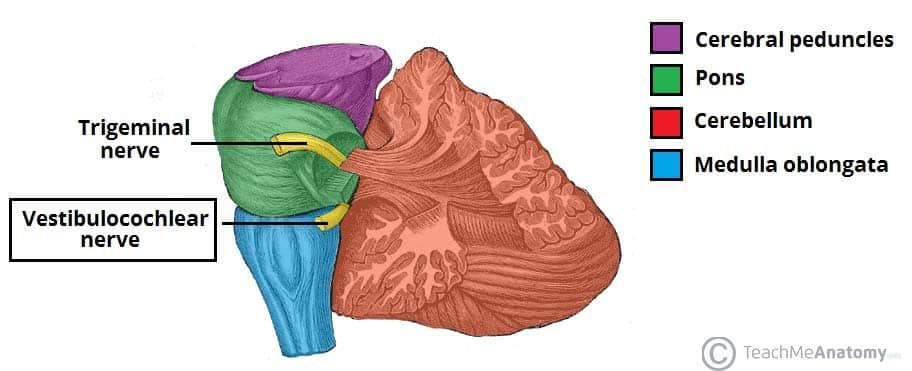
- Commonly located within the internal acoustic canal and can extend into the cerebellopontine angle (most common tumor of the cerebellopontine angle)
Etiology
Pathophysiology
Clinical features
- Early symptoms: as a result of tumor expansion into the internal acoustic canal (internal auditory meatus), causing pressure on the vestibulocochlear nerve (CN VIII)
- Cochlear nerve involvement
- Unilateral sensorineural hearing loss (most common symptom)
- Tinnitus
- Vestibular nerve involvement
- Dizziness
- Cochlear nerve involvement
- Late symptoms: caused by pressure of adjacent structures within the cerebellopontine angle
- Trigeminal nerve (CN V) involvement: paresthesia (numbness), hypoesthesia (decreased sensation), and/or unilateral facial pain
- Facial nerve (CN VII) involvement: peripheral, unilateral facial weakness that can progress to paralysis
- Compression of structures in posterior fossa
Diagnostics
Pathology
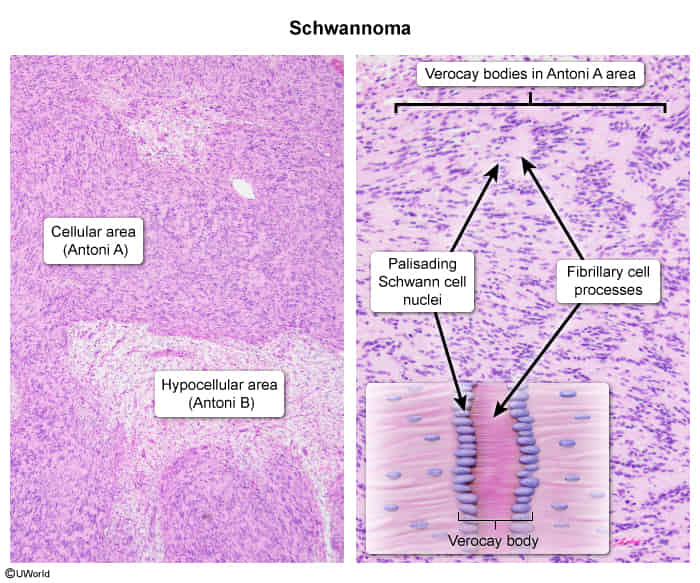
- Spindle cells (fibroblasts) in palisades (Antoni A tissue) alternating with myxoid hypocellular areas (Antoni B tissue)
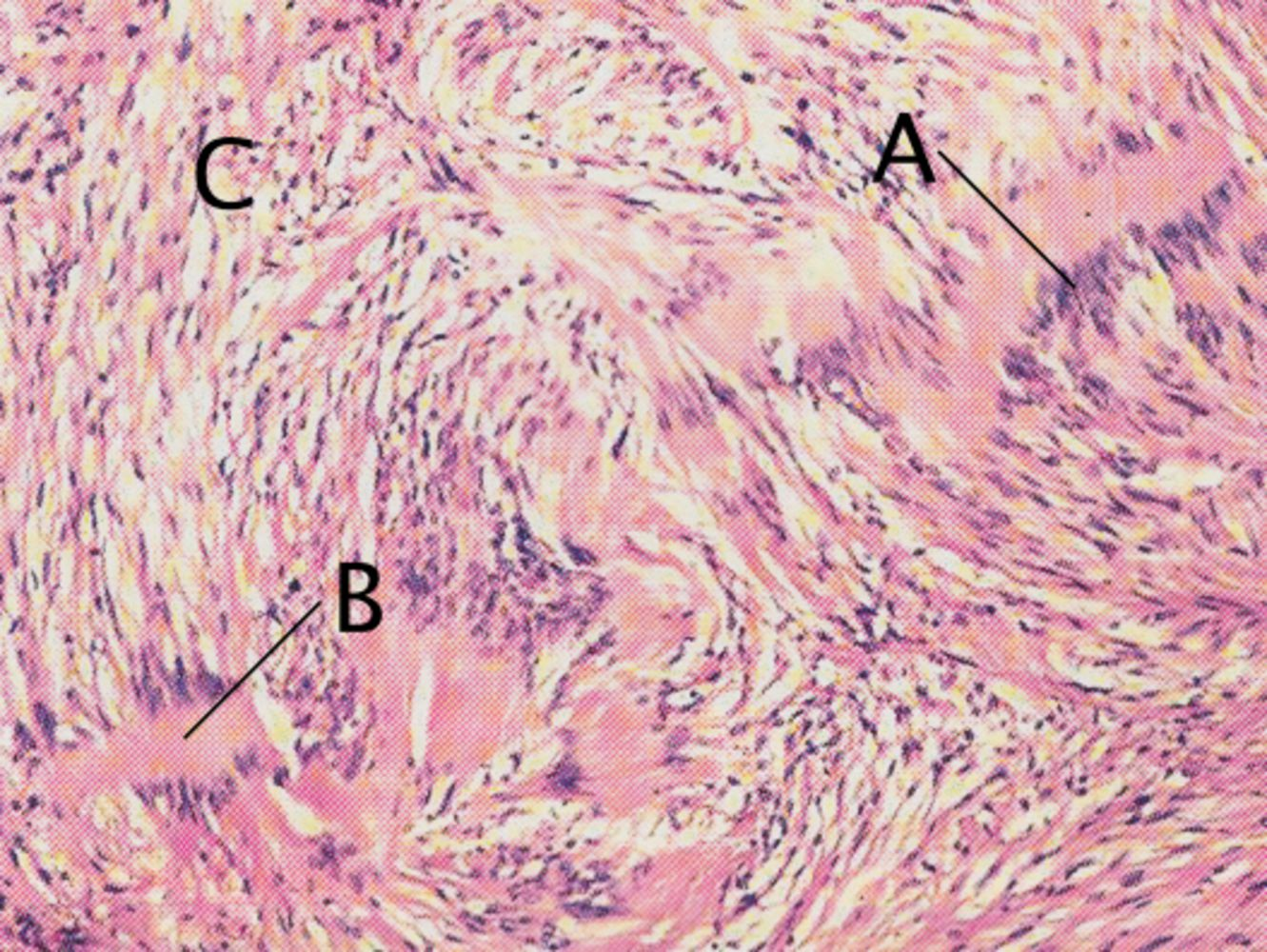
- A characteristic finding of neuromas is the simultaneous occurrence of areas with densely packed nuclei (palisade pattern; A) and scattered or anuclear areas (B). There is also a large number of vacuolated cells (C).
- S-100 positive
- S-100 can be seen in melanoma, schwannoma, Langerhans cell histiocytosis