Consuming gliadin from grains such as wheat, rye, and barley leads to an autoimmune reaction within the small intestinal wall.
Pathophysiology
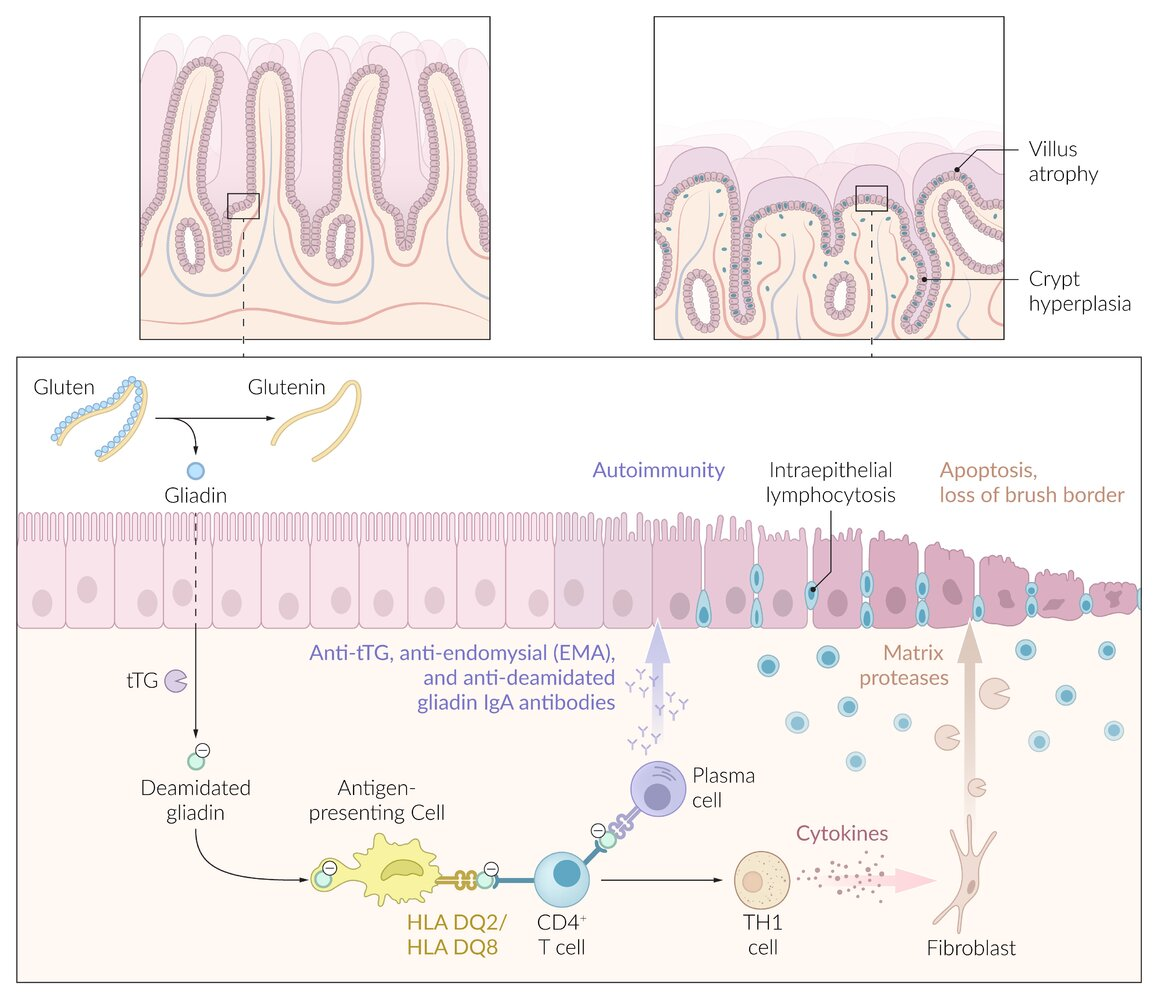
Symptoms manifest when a genetically predisposed individual develops an immunological response to gliadin, an alcohol-soluble fraction of gluten.
Consumption of food containing gluten → tissue transglutaminase is released → modifies gliadin from gluten proteins → pathogenic T cells react to and are activated by modified gliadin → mediate chronic intestinal inflammation → epithelial damage resulting in villous atrophy, crypt hyperplasia, and loss of brush border → impaired resorption of nutrients in the small intestine (especially in the distal duodenum and proximal jejunum) → malabsorption symptoms
Transglutaminases play a role in forming extensively cross-linked proteins (e.g., elastin, coagulation by factor XIII).
Neuropsychiatric symptoms: peripheral neuropathies (numbness, burning and tingling of the hands and feet) , headache, ataxia, depression, irritability
Commonly associated with autoimmune diseases
Diagnostics
Laboratory studies
IgA tissue transglutaminase antibody (tTG IgA): initial test
Total IgA
Indicated for all patients because of the high prevalence of IgA deficiency in patients with celiac disease (approx. 2–3%)
Both celiac disease and selective IgA deficiency have strong associations with specific HLA genes, particularly HLA-DQ2 and HLA-DQ8.
If patients have low IgA, perform further IgG-based testing.
Deamidated gliadin peptide
IgG-based testing: indicated in IgA deficiency or discordant biopsy and serology
IgG-tissue transglutaminase (tTG IgG)
IgG deamidated gliadin peptide (DGP IgG)
IgA-based testing: IgA deamidated gliadin peptide (DGP IgA)
Anti-endomysial antibody (EMA): Potential second-line confirmatory test (high-specificity)
Celiac disease is not associated with elevated systemic inflammatory markers (eg, C-reactive protein, erythrocyte sedimentation rate), since it’s limited.
Endoscopy
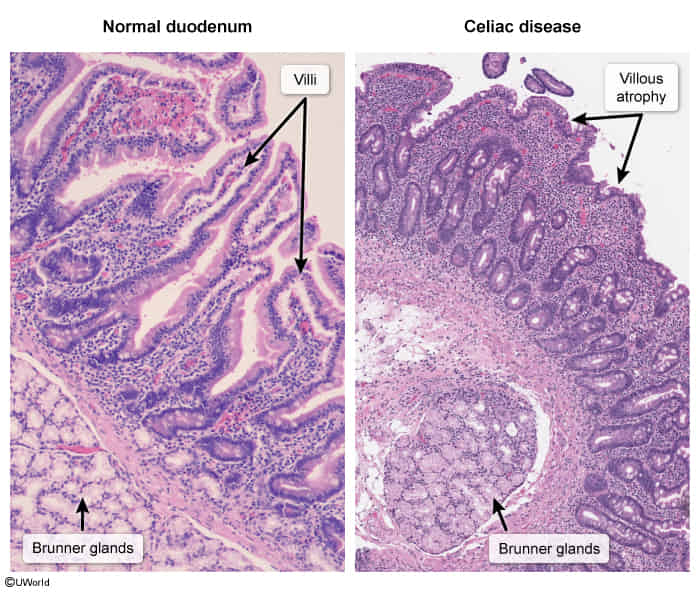
EGD with small intestine biopsy (confirmatory test)
Intraepithelial lymphocytic infiltration
Crypt hyperplasia
Villous atrophy
Differential diagnostics
Tropical sprue
Definition: A disease characterized by chronic diarrhea with subsequent malabsorption in association with a stay in the tropics or subtropics.
Epidemiology: occurs in residents of the tropics and subtropics or in travelers returning from these areas (after trips lasting several weeks)
Etiology: exact cause not known; most likely due to bacterial infection that leads to structural damage of the intestinal mucosa
Clinical features: similar to Celiac disease
Diagnostics
Endoscopy of the small bowel and biopsy: villous atrophy, elongated crypts, presence of inflammatory cells (plasma cells, lymphocytes, eosinophils)
Treatment: tetracycline in combination with folic acid for 3–6 months
Treatment
Strict, lifelong gluten-free diet
Abstain from products containing wheat, rye, barley, or spelt.