Deficiency of vWF, cause mixed platelet and coagulation disorders
Epidemiology
Most common congenital bleeding disorder.
Etiology
Acquired von Willebrand disease (aVWD)
- Lymphoproliferative and myeloproliferative diseases (e.g., multiple myeloma, monoclonal gammopathies, lymphoma, essential thrombocythemia)
- Autoimmune diseases (e.g., SLE)
- Cardiovascular defects (e.g., ventricular septal defect, aortic stenosis)
- These conditions lead to increased shear stress in blood vessel which can result in increased degradation of vWF.
- Hypothyroidism
- Side effects of certain drugs (e.g., valproic acid)
Pathophysiology
- Von Willebrand factor (vWF): plasma protein that is synthesized by and stored in endothelial cells (in Weibel-Palade bodies) and platelets (in α-granules)
- Mediates platelet adhesion and aggregation
- Binds factor VIII (and thereby prevents its degradation)
Deficiency or dysfunction of vWF leads to: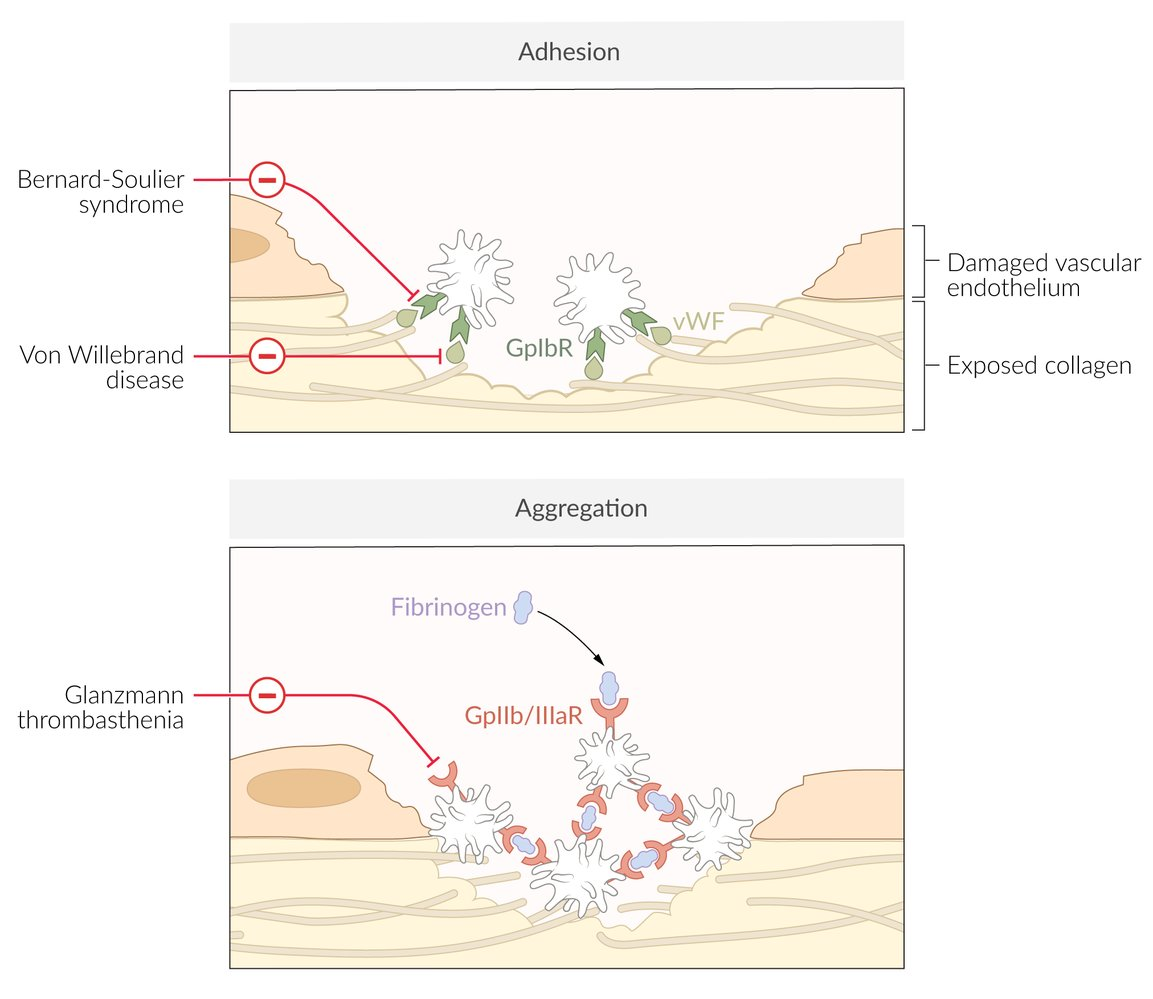
- Dysfunctional platelet adhesion → impaired primary hemostasis
- Reduced binding of factor VIII → increased degradation → ↓ factor VIII activity → impaired intrinsic pathway of secondary hemostasis
Clinical features
- Predominantly mucocutaneous bleeding.
- Common Sx: Epistaxis (nosebleeds), gingival bleeding, easy bruising, petechiae.
- Menorrhagia (heavy menstrual bleeding) is very common in female pts.
- Prolonged bleeding after minor cuts, dental procedures, or surgery.
- Severe forms (Type 3) can present similarly to hemophilia with hemarthrosis (joint bleeding) and soft tissue hematomas.
Diagnostics
- Platelet Count: Normal. The defect is in platelet function (adhesion), not number.
- Bleeding Time: Increased due to impaired platelet plug formation.
- Prothrombin Time (PT): Normal, as the extrinsic pathway is unaffected.
- Partial Thromboplastin Time (PTT): Normal or Increased. PTT may be elevated because ↓ vWF leads to ↓ Factor VIII levels.
- The PTT test is relatively insensitive to mild deficiencies of clotting factors. For the PTT to become prolonged, Factor VIII activity must typically drop below 30-40% of normal.
- Definitive Tests:
- Ristocetin Cofactor Assay: This is the key functional test. It measures vWF’s ability to agglutinate platelets in the presence of the antibiotic ristocetin. In vWD, there is ↓ or absent agglutination. This test is abnormal in all types except 2N.
- vWF Antigen: Measures the quantity of vWF protein.
- Factor VIII Activity: Often decreased.
Treatment
- Desmopressin (DDAVP): stimulates vWF release from endothelial cells
- Best initial treatment for mild or moderate symptoms (typically type 1 and, sometimes, type 2)
- Not effective for type 3
- Has a minimal effect on the V1 vasopressin receptor. Therefore won’t cause vasoconstriction.
- Concentrates containing vWF and factor VIII: indicated for severe bleeding, as prophylaxis for surgical procedures and if DDAVP treatment is ineffective