Epidemiology
- General: Approx. 90–95% of adults are EBV-seropositive worldwide.
- Peak incidence (of symptomatic disease): 15–24 years of age
Etiology
- Pathogen: Epstein-Barr virus (EBV), also called human herpesvirus 4 (HHV-4)
- Transmission: Infectious mononucleosis spreads via bodily secretions, especially saliva. Therefore, it is also called kissing disease.
Pathophysiology
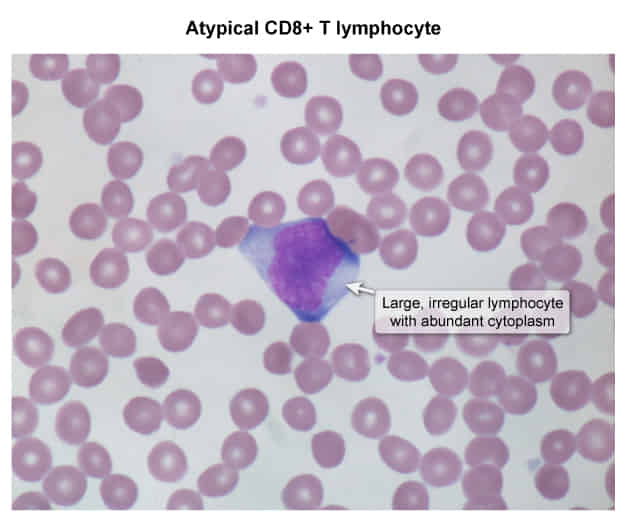
- EBV infects B lymphocytes in mucosal epithelium (e.g., oropharynx, cervix) via the CD21 receptor → infected B lymphocytes induce a humoral (B-cell) as well as a cellular (T-cell) immune response → an increased concentration of atypical lymphocytes in the bloodstream, which are CD8+ cytotoxic T cells that fight infected B lymphocytes
- Atypical lymphocytes are not infected by virus; they react to infected cells. They contain cytotoxic granules composed of perforin (creates holes in the infected cell’s membrane) and granzymes (enter the cytoplasm of infected cells and trigger cell death)
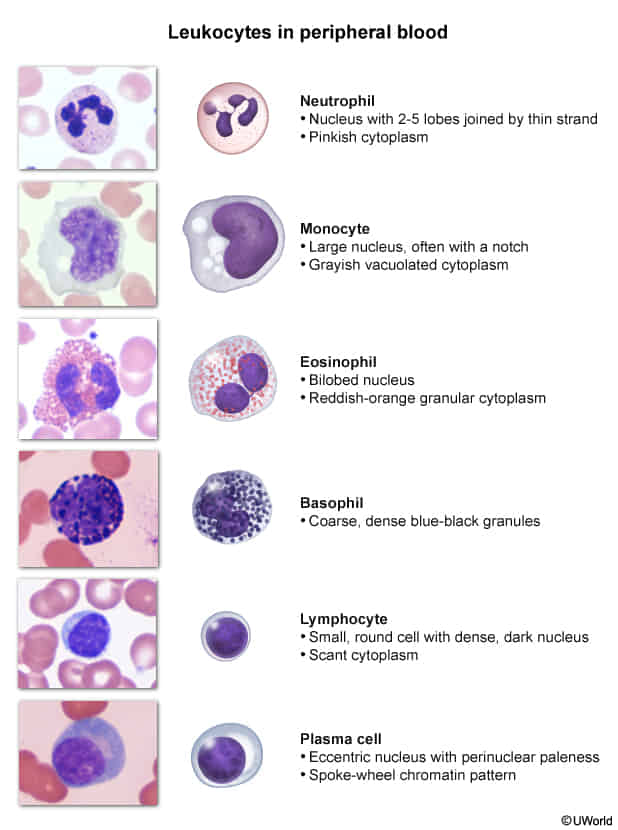
- The name “mononucleosis” is derived from the monocyte-like appearance of (atypical) lymphocytes under the microscope.
- The T-cell response is crucial for overcoming the infection. However, if the response is not sufficient (e.g., in HIV patients), B cells may proliferate uncontrollably and increase the risk of complications. For example, the high rate of proliferation increases the risk of oncogenic mutations that lead to the development of B-cell lymphomas.
Clinical features
- Incubation period: ∼ 6 weeks
- Clinical course
- Symptoms typically occur in adolescents and young adults and last for 2–4 weeks.
- Signs and symptoms
- Splenomegaly, fever, fatigue, malaise
- Pharyngitis and/or tonsillitis (reddened, enlarged tonsils covered in pus), palatal petechiae
- Bilateral cervical lymphadenopathy (especially posterior) that may become generalized and can, in severe cases, lead to airway obstruction
- Abdominal pain
- Possibly hepatomegaly and jaundice
- Maculopapular rash (similar to measles): The rash is caused by the infection itself in about 5% of cases but is most commonly associated with the empiric administration of aminopenicillin (e.g., ampicillin, amoxicillin)
Warning
Splenomegaly can lead to a potentially life-threatening splenic rupture!
Diagnostics
- Monospot test
- Detects heterophile antibodies produced in response to EBV infection using RBCs from sheep or horses
- The mechanism remains unclear; EBV either induces a humoral response to heterophile antigens or stimulates nonspecific polyclonal activation of B cells.
- Patient’s serum is mixed with a solution of sheep/horse RBC in vitro
- Positive test: cross-reaction between heterophile antibodies and sheep/horse RBCs → agglutination
- Negative test
- No heterophile antibodies present → no cross-reaction → no agglutination
- In some cases, the test can show negative results if it is performed too soon (i.e. within the first 1–2 weeks after symptom onset) and antibodies have not developed yet.
- Specificity of ∼ 100%, sensitivity of 85%
- Detects heterophile antibodies produced in response to EBV infection using RBCs from sheep or horses
- Peripheral smear: lymphocytosis with > 10% atypical lymphocytes (in some cases, up to 90%)
- Since EBV typically causes a latent infection of B cells, only minimal amounts of EBV-specific antigens circulate in an immunocompetent host; therefore, blood tests for such antigens are insensitive to latent EBV infection.
Differential diagnostics
- Mononucleosis-like syndromes
- Streptococcal pharyngitis, tonsillitis
- Acute HIV infection
- Viral hepatitis
- CMV infection
- Toxoplasmosis
Treatment
Complications
- Post-transplant lymphoproliferative disorder: a group of aggressive and rapidly progressive complications of solid organ transplantation and allogeneic hematopoietic stem cell transplantation
- Associated with EBV reactivation in patients with severe immunosuppression (e.g., post-transplantation medications)
- Clinical features: fever, weight loss, fatigue, lymphadenopathy, hepatosplenomegaly
- Commonly progresses to B-cell lymphoma: poor prognosis
- Treatment: reduce immunosuppressive therapy