Epidemiology
- Sex: ♂ > ♀
- Age: more common in children
- 90% of affected individuals < 10 years
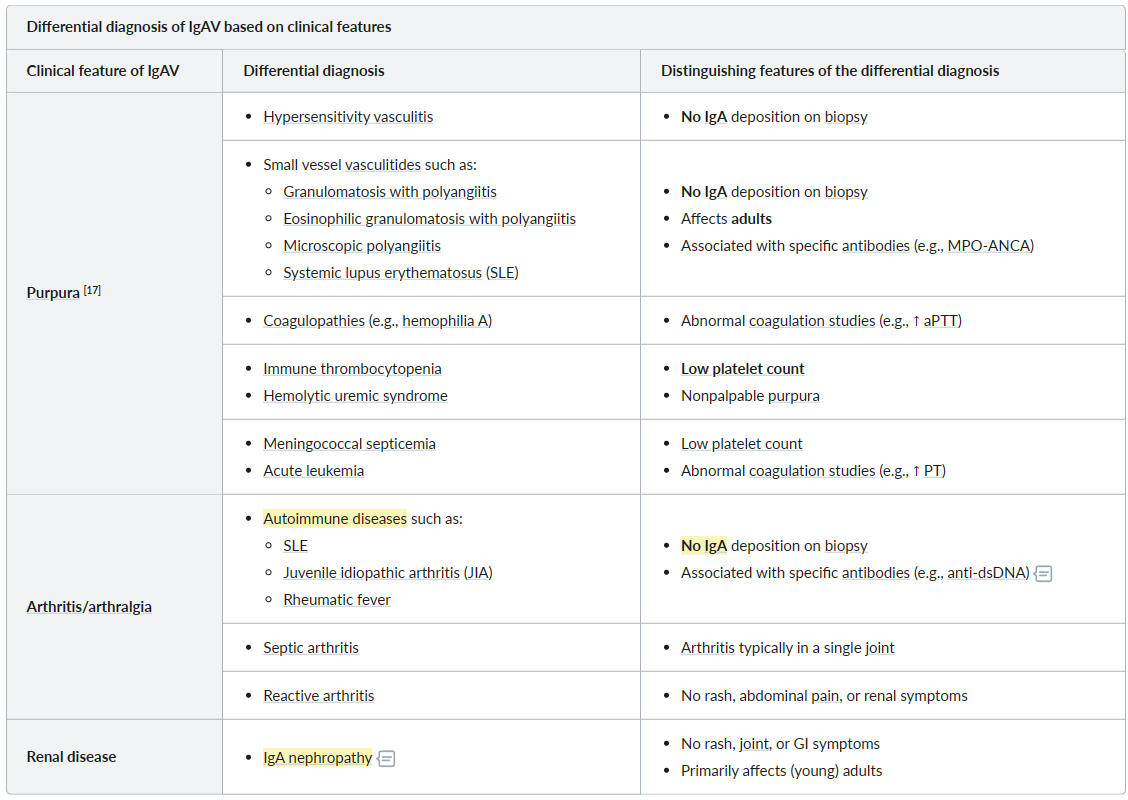
- Other small vessel vasculitides mainly affect adults
Etiology
- Preceding infection
- Up to 90% of cases are preceded by viral or bacterial infection 1–3 weeks prior.
- Most commonly an upper respiratory tract infection caused by group A Streptococcus
- IgA nephropathy
- Drugs
Pathophysiology
Hypothesized pathophysiological mechanism: exposure to allergen/antigen (e.g., infection, drugs) → stimulation of IgA production → deposition of IgA immune complexes in vascular walls (e.g., in the skin, GI tract, joints, kidneys) → activation of complement → vascular inflammation and damage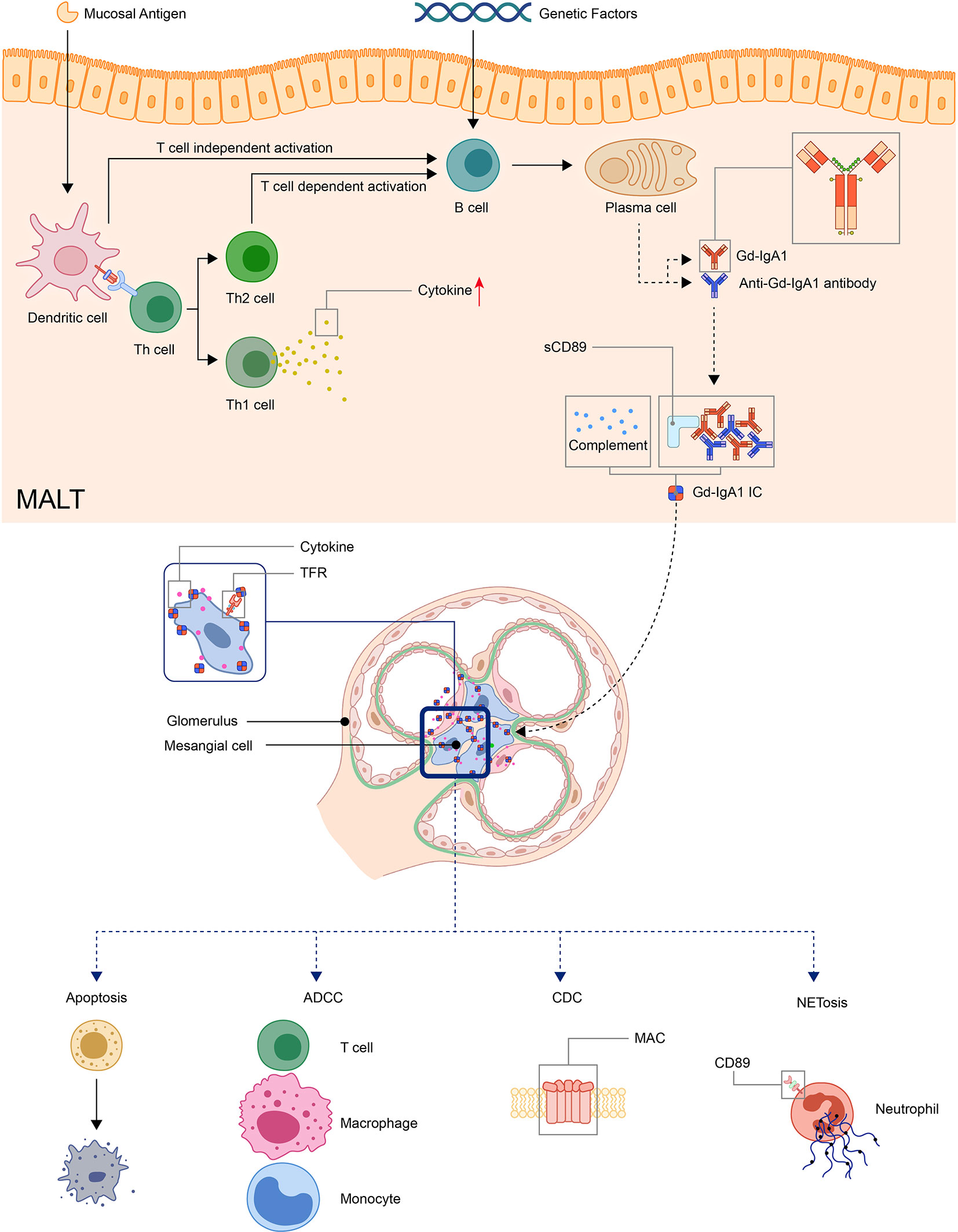
Clinical features
Key features
- Triad of palpable purpura, arthralgias, and abdominal pain in children.
- Afebrile, which differentiates its with infectious disease
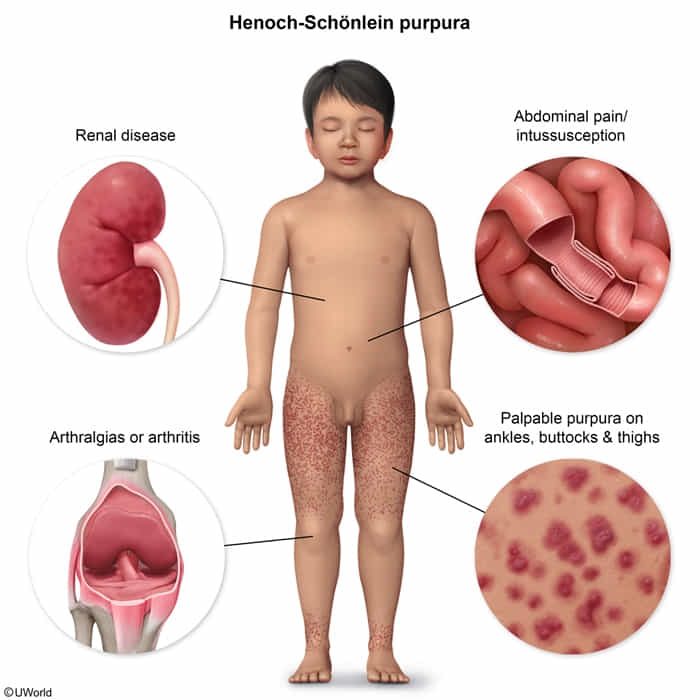
- The classic tetrad includes:
- Palpable Purpura: Present in nearly all patients, typically non-pruritic and symmetrically distributed on the lower extremities and buttocks. The rash begins as erythematous or urticarial lesions that evolve into palpable purpura.
- Arthritis/Arthralgia: Occurs in ~75% of patients, presenting as transient, non-destructive joint pain and swelling, most commonly affecting the ankles and knees.
- Abdominal Pain: Affects 50-75% of patients; it is often colicky. Can be associated with nausea, vomiting, and GI bleeding (melena or hematemesis).
- Renal Disease: Occurs in 40-50% of patients and is the main determinant of long-term prognosis. It can range from microscopic hematuria and mild proteinuria to a rapidly progressive glomerulonephritis.
- Scrotal edema can also be seen, particularly in young boys.

Tip
- IgA Nephropathy and IgA Vasculitis (Henoch-Schönlein Purpura) are considered different clinical presentations of the same biological process.
- IgA Nephropathy = Renal-limited form.
- IgA Vasculitis = Systemic form involving skin, joints, GI tract, and kidneys.
Tip
IgAV is an important differential diagnosis to consider in children with a limp.
Diagnostics
Biopsy
- IgA and C3 complex deposition (hallmark) in small vessels of the superficial dermis
- ANCA negative vasculitis