Etiology
Idiopathic
Infectious
Most commonly viral (e.g., coxsackie B virus) Bacterial (e.g., Staphylococcus spp., Streptococcus spp., or M. tuberculosis )
Myocardial infarction
Postinfarction fibrinous pericarditis: within 1–3 days as an immediate reaction Dressler syndrome: weeks to months after an acute myocardial infarction
Postoperative (postpericardiotomy syndrome): due to blunt or sharp trauma to the pericardium
Uremia: e.g., due to acute or chronic renal failure
Accumulated toxins promote inflammation.
Radiation
Neoplasms (e.g., Hodgkin lymphoma )
Autoimmune connective tissue diseases (e.g., rheumatoid arthritis , SLE , scleroderma )
Trauma
Classifications
Serous Pericarditis
Fibrous or Fibrinous Pericarditis
Most common pericarditis MI (Dressler syndrome)
Rheumatic fever Uremia TB pericarditisMalignancy involvement
Pericardial surface covered by shaggy, fibrinous exudate
“Bread and Butter” appearance
Purulent (Suppurative) Pericarditis
Pyogenic bacteria (Staphylococci, Streptococci, Pneumococci)
Direct extension / hematogenous or lymphatic spread / direct implant
Severe acute infection
Pericardial surface covered by purulent exudate and infiltrated by neutrophils
Hemorrhagic Pericarditis
Malignancy involvement
TB pericarditisSevere acute infection
Admixture of inflammatory effusion with blood
Clinical features
Acute pericarditis
Chest Pain (CP) : Pleuritic, sharp, retrosternal.Positional : Worse when supine; relieved by leaning forward .Radiation : Trapezius ridges (pathognomonic; phrenic nerve irritation).Physical Exam (PE) : Pericardial Friction Rub (high-pitched, scratching/velcro sound; heard best at LLSB with pt leaning forward during expiration).
Chronic pericarditis
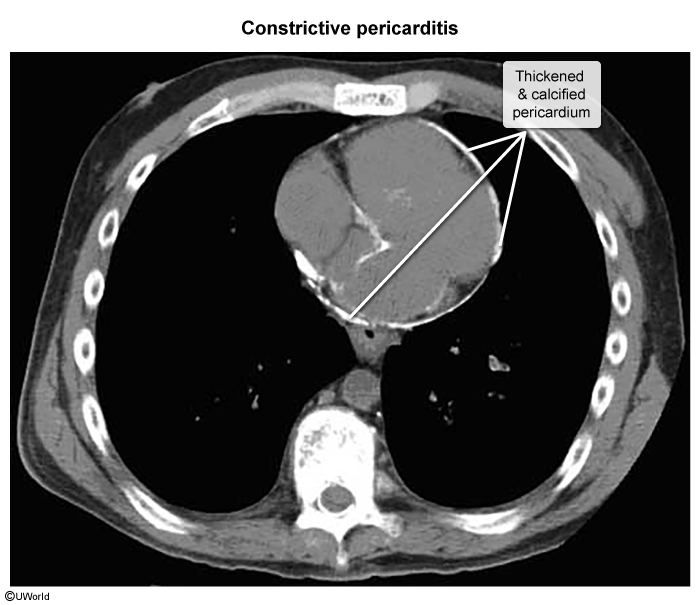
Constrictive pericarditis
Symptoms of fluid overload (i.e., backward failure)
Jugular vein distention, ↑ jugular venous pressure
Kussmaul Sign : Paradoxical rise in JVD with inspiration (impaired RV filling).Pericardial Knock : High-frequency early diastolic sound (caused by sudden cessation of ventricular filling). c
Differ from S3, which is low-frequency early diastolic sound
Diagnostics
Acute pericarditis
Clinical Dx : Requires ≥2 of 4: (1) Characteristic CP, (2) Friction rub, (3) EKG changes, (4) New/worsening pericardial effusion.Initial/Screening (EKG) :
Diffuse ST-elevation (concave/up-sloping) and PR-segment depression (highly specific). c Note: aVR will show ST-depression and PR-elevation.
Key Labs : ↑ ESR, ↑ CRP, mild leukocytosis. ↑ Troponin I/T suggests perimyocarditis .Imaging :
CXR : Usually normal. “Water-bottle heart” if large effusion (>200mL) present.Echocardiogram : Initial test to rule out effusion or tamponade; often normal in uncomplicated pericarditis.
Chronic pericarditis
Imaging
CT and cardiac MRI
Pericardial thickening > 2 mm Calcifications
Treatment
First-line (Idiopathic/Viral) : NSAIDs (Ibuprofen or Indomethacin) + Colchicine (colchicine significantly ↓ recurrence rate).Second-line / Refractory : Corticosteroids (Prednisone). Note: Avoid steroids as first-line unless NSAIDs are contraindicated (e.g., pregnancy, severe renal disease) or if etiology is autoimmune, due to high risk of recurrence. Etiology-Specific Variants :
Post-MI : Aspirin + Colchicine (Avoid other NSAIDs & steroids; they impair myocardial scar formation and ↑ risk of ventricular free wall rupture).Uremic Pericarditis : Hemodialysis (NSAIDs/colchicine are ineffective and contraindicated).