Function
Motor (somatic)
- Eyelid opening (indirect): levator palpebrae superioris muscle
- Eye movement
- Superior rectus muscle: elevation, intorsion, and adduction
- Inferior rectus muscle: depression and extorsion
- Medial rectus muscle: adduction
- Inferior oblique muscle: extorsion, elevation, and abduction
Motor (parasympathetic)
- Pupillary constriction
- Pupillary sphincter (Edinger-Westphal nucleus and muscarinic receptors)
- Efferent limb of the pupillary light reflex
- Accommodation: ciliary muscle
Tip
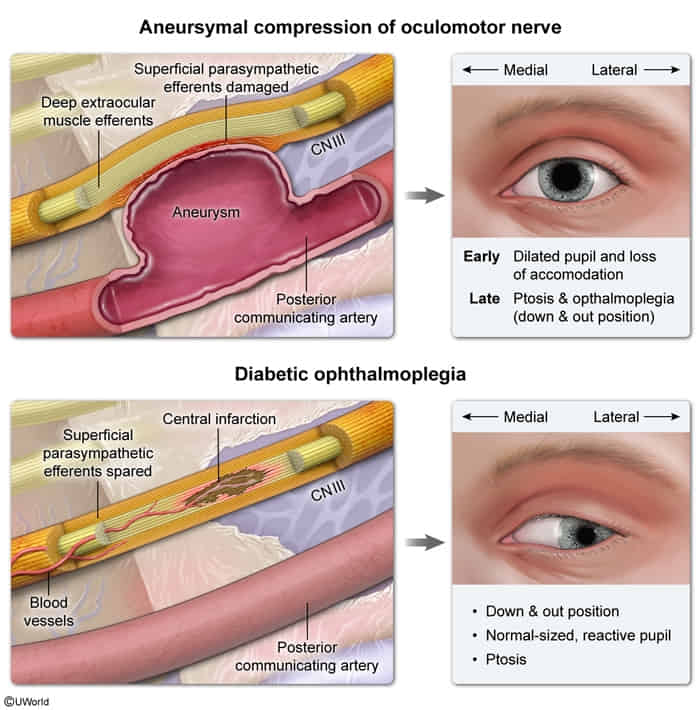
Parasympathetic fibers of CN III are located superficially and motor fibers are located centrally. Parasympathetic fibers are more susceptible to compressive lesions (e.g., uncal herniation, aneurysm of the posterior communicating artery). Motor fibers are more susceptible to ischemia (e.g., vasculitis, diabetes, atherosclerosis).
Etiology
Basilar segment
The basilar segment is the only region where the oculomotor nerve is not accompanied by other cranial nerves.
Cause
- Aneurysm of the posterior communicating artery
- Clinical features
- Headache
- Paralytic squint
- Pupillary involvement: nonreactive, dilated pupil (blown pupil)
- Clinical features
- Transtentorial herniation (uncal herniation)
- Clinical features
- Abducens nerve palsy
- CN VI is the first cranial nerve to be affected by an elevated ICP.
- Features of elevated intracranial pressure (e.g., coma, blown pupil)
- Hutchinson pupil
- Abducens nerve palsy
- Clinical features
Pathophysiology
Clinical features
- Horizontal diplopia that worsens when the head is turned away from the side of the lesion
- Ptosis
- Due to levator palpebrae superioris muscle weakness
- Light sensitivity
Diagnostics
- Assessment of extraocular muscle function : Lesions of the motor portion typically produce paralytic squint.
- Down-and-out gaze: affected eye looks outwards (exotropia) and downwards (hypotropia)
- This type of squint occurs because of the action of the lateral rectus muscle and the superior oblique muscle, and it is only seen in individuals with isolated oculomotor nerve palsy.
- Adduction weakness
- Down-and-out gaze: affected eye looks outwards (exotropia) and downwards (hypotropia)
- Assessment of pupillary response (afferent: CN II; efferent: CN III)
- Lesions of the autonomic (parasympathetic) portion result in loss of the pupillary reflex.
Tip
Impaired pupillary reaction with relative sparing of motor function is typically seen in compressive lesions. Prominent motor dysfunction with sparing of the pupil is typically seen in ischemic lesions. See Diabetic neuropathy > Diabetic CN III mononeuropathy