Epidemiology
Peak incidence: neonatal period (first 30 days of life) and during puberty (10–14 years)
Etiology
- Idiopathic
- Iatrogenic
- Following a testicular procedure with incorrect positioning of testis
Pathophysiology
- Testicular torsion is a sudden twisting of the spermatic cord (and vascular pedicle) associated with a poorly secured testis.
- Because of a congenital abnormality in which the tunica vaginalis attaches to the superior pole of the testis (bell-clapper deformity) → increased mobility of testis within tunica vaginalis, with possible abnormal transverse lie of testis → torsion of the testis (along the spermatic cord)
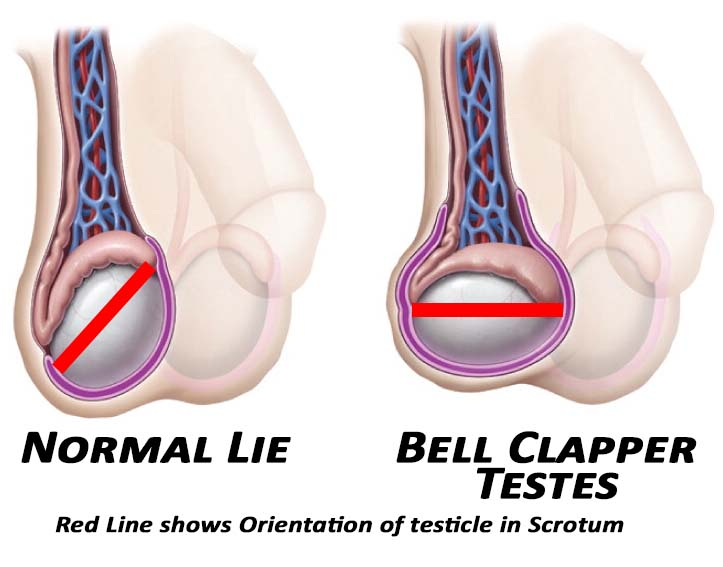
- Because of a congenital abnormality in which the tunica vaginalis attaches to the superior pole of the testis (bell-clapper deformity) → increased mobility of testis within tunica vaginalis, with possible abnormal transverse lie of testis → torsion of the testis (along the spermatic cord)
- Torsion results in venous engorgement with consequent arterial compromise, tissue ischemia, and possible infarction.
- Irreversible damage occurs after 6–12 hours of torsion.
Clinical features
- Abrupt onset of severe testicular pain and/or pain in the lower abdomen
- swollen and tender testis
- Nausea and vomiting
- Abnormal position of the testis
- Scrotal elevation (high-riding testis)
- Absent cremasteric reflex
- Impairment of nerves within the cord
- Negative Prehn sign
- A physical examination finding in which elevation of the scrotum relieves testicular pain. A positive Prehn sign is associated with epididymitis; a negative Prehn sign is associated with testicular torsion.
- Elevation of the scrotum can improve venous drainage and relieve edema in epididymitis; but cannot relieve ischemia in testicular torsion.
Tip
- Testicular torsion: negative Prehn sign, negative cremasteric reflex
- Epididymitis: positive Prehn sign, positive cremasteric reflex