Spirochetes invade the body → disseminate systemically within hours → bind to endothelial cells → inflammatory reaction → endarteritis and perivascular inflammatory infiltrates
May be obliterating if reactive endothelial hyperproliferation occurs and results in ischemia and necrosis.
Clinical features
Primary syphilis
Primary lesion (chancre)
Typically starts out as a solitary, raised papule (usually on the genitals)
Evolves into a painless, firm ulcer with indurated borders and smooth base
Resolves spontaneously within 3–6 weeks, typically without scarring
Nontender regional lymphadenopathy (e.g., involvement of the inguinal lymph nodes in genital primary syphilis)
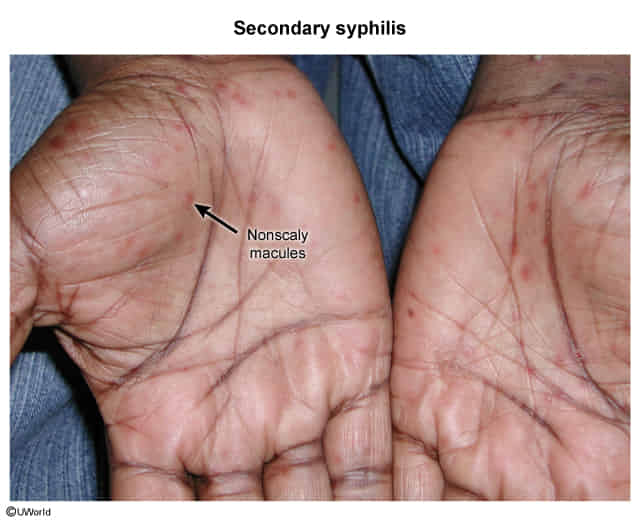
Secondary syphilis
Disseminated disease due to the systemic spread of the spirochetes, inducing an immunologic reaction
Begins approx. 2–12 weeks after primary infection and typically lasts 2–6 weeks